

This week, the most rapid period of weight gain in your entire pregnancy begins.
Not the beginning of weight gain – that has been happening for months. The beginning of the most rapid phase. From Week 35 until birth, your baby gains approximately 8 to 12 ounces every single week. The fat depositing right now is going specifically to the places that matter most for a newborn’s survival: the shoulders, the cheeks, the thighs – the places that will help regulate temperature, cushion the delivery, and make your baby look like the round, soft infant you have been imagining.
Your baby’s kidneys are also fully developed this week. Every waste product passing through your baby’s body is being processed, filtered, and returned to the amniotic fluid as urine. A complete, functional organ system – finished.
And your baby’s brain, while continuing to grow rapidly, has reached two-thirds of its final term weight. The remaining third – gained almost entirely in the last five weeks – is less about new structures and more about the connectivity between them. The neurons are mostly there. What is being built now is the wiring between them.
Five weeks from your due date. Here is everything happening at 35 weeks pregnant.

Contents
- 1 Quick Summary: 35 Weeks Pregnant
- 2 What’s Happening in Your Body at 35 Weeks Pregnant
- 3 Baby Development at 35 Weeks Pregnant
- 4 The Brain at 35 Weeks – What Two-Thirds Actually Means
- 5 The Group B Strep Test – What Happens This Week
- 6 The Mucus Plug – What It Is and What Losing It Means
- 7 35 Weeks Pregnant Symptoms
- 8 Late Preterm Birth – What 35 Weeks Actually Means
- 9 Nutrition at 35 Weeks Pregnant
- 10 Partner Tips for Week 35
- 11 35 Weeks Pregnant Checklist
- 12 Frequently Asked Questions – 35 Weeks Pregnant
- 12.1 What trimester is 35 weeks pregnant?
- 12.2 How many months is 35 weeks pregnant?
- 12.3 How much does a baby weigh at 35 weeks pregnant?
- 12.4 Can a baby survive at 35 weeks?
- 12.5 What is the GBS test at 35 weeks pregnant?
- 12.6 What does losing the mucus plug look like at 35 weeks?
- 12.7 What is late preterm birth and what are the risks?
- 12.8 Why does my baby feel less active at 35 weeks?
- 13 Looking Ahead: 36 Weeks Pregnant
Quick Summary: 35 Weeks Pregnant
| Detail | Info |
| Baby size | Honeydew melon – ~46-47 cm, ~2.4-2.6 kg (5.3-5.7 lbs) |
| Trimester | Third trimester – Week 8 of T3 |
| Months pregnant | Late 8th month / nearly 9 months |
| Weeks remaining | 5 weeks to go |
| Top milestone | Most rapid weight gain begins + kidneys fully developed |
| This week’s action | GBS test this week or next + shift to weekly appointments |
What’s Happening in Your Body at 35 Weeks Pregnant

At 35 weeks pregnant, your uterus has grown to approximately 500 to 1,000 times its original size – a number that sounds impossible but that your body can confirm is entirely real. It now extends roughly 6 inches above your belly button and is pressing against essentially every organ in your abdominal cavity simultaneously.
Your appointments are shifting. Between Weeks 35 and 36, most providers move from biweekly to weekly appointments. This is not a sign of concern – it is a sign that you are entering the final phase of pregnancy, and your provider wants more frequent monitoring as your due date approaches.
Weight gain at this stage is approximately half a pound per week for you – and approximately half of that is your baby. At 35 weeks pregnant, total weight gain typically falls between 24 and 29 pounds, though this range varies meaningfully based on your starting weight and your provider’s specific guidance.
What to expect at your Week 35 appointment:
- Blood pressure and urine protein – preeclampsia monitoring continues
- Fundal height – should be approximately 33-37 cm
- Baby’s heartbeat
- Baby’s position – by Week 35, the vast majority of babies are head-down
- GBS swab test – vaginal and rectal swab, results in 24-48 hours
- Discussion of labor signs – what to watch for and when to call
- Review of your birth plan if you haven’t shared it yet
- Confirmation that hospital bag is packed and route is known
Baby Development at 35 Weeks Pregnant

At 35 weeks pregnant, your baby measures approximately 46-47 cm from head to heel and weighs around 2.4 to 2.6 kg – roughly the size and weight of a large honeydew melon.
| Detail | Measurement |
| Length | ~46-47 cm (about 18-18.5 inches) |
| Weight | ~2.4-2.6 kg (approx. 5.3-5.7 lbs) |
| Size comparison | Large honeydew melon |
| Heart rate | 110-160 bpm |
| Most rapid weight gain | Begins this week – 8-12 oz per week |
Key developments this week:
- Most rapid weight gain begins: Week 35 marks the start of the fastest weight gain phase of the entire pregnancy. Baby gains 8-12 ounces per week from now until birth – almost entirely fat deposited at the shoulders, cheeks, and limbs. This fat serves a specific purpose: keeping your newborn warm in the hours after delivery when they lose the temperature regulation of the womb.
- Kidneys fully developed: Your baby’s kidneys are completely developed and fully functional. They are processing waste, producing urine, and contributing to the amniotic fluid that surrounds your baby. This is a significant organ milestone – the kidneys will need to function immediately and independently from the moment of birth.
- Brain at two-thirds of term weight: Your baby’s brain now weighs approximately two-thirds of what it will weigh at 39-40 weeks. The remaining third is gained almost entirely in the final five weeks – and this final phase is less about new brain structures and more about the density of neural connections being formed. More connections mean faster processing, stronger reflexes, and better coordination at birth.
- Fat depositing at the shoulders specifically: Fat is accumulating throughout the body but with particular concentration around the shoulders. This shoulder fat serves both thermoregulation and delivery purposes – it cushions the passage of the shoulders through the birth canal, which is often the widest part of the delivery.
- Hearing at near-adult sharpness: Your baby’s hearing is now fully developed and responds most strongly to high-pitched sounds. Your baby can distinguish between voices, between music and speech, and between familiar and unfamiliar sounds. The auditory pathways that began encoding patterns at Week 34 are now running at near-full sensitivity.
- Lanugo almost completely gone: The fine downy hair that covered your baby’s skin throughout the second trimester has almost entirely shed. Traces may remain on the shoulders and back at birth – this is normal and falls away within days.
- Grasp reflex coordinating: Your baby can now grip firmly. The grasp reflex – which is tested in the newborn examination – is becoming strong and coordinated. Some babies grip the umbilical cord during this period.
- Digestive system ready: While the digestive system does not activate until after birth (the placenta handles nutrition), all the organs and mechanisms needed for digestion are assembled and waiting. The intestines, liver, pancreas, and stomach are ready to begin their post-birth function.
The Brain at 35 Weeks – What Two-Thirds Actually Means
Most pregnancy guides note that the brain weighs about two-thirds of its term weight at 35 weeks. Very few explain what the remaining third actually consists of – and the answer is what makes the final five weeks so developmentally significant.
The major brain structures – the cerebral cortex, cerebellum, brainstem, limbic system – are all present and largely assembled. What the brain is doing from Week 35 through birth is not building new rooms. It is furnishing the ones that already exist.
The final third of brain weight is gained through:
- Synaptogenesis – the formation of new synaptic connections between neurons. The density of these connections determines processing speed and learning capacity.
- Myelination – the continued coating of nerve fibers with myelin, which dramatically increases nerve signal speed. Myelination continues well into early childhood but accelerates sharply in the final weeks of pregnancy.
- Glial cell proliferation – supporting cells that nourish neurons, regulate their environment, and assist in signal transmission continue multiplying through birth.
- Cortical folding – the gyri and sulci forming since Week 28 continue developing, adding surface area and increasing the number of neurons the cortex can contain.
This is why late preterm births – between 35 and 37 weeks – carry specific neurological risks that were not present at 34 weeks. The brain is present and functional, but the final connectivity phase is incomplete. Babies born at 35 weeks have higher rates of feeding difficulties, temperature regulation challenges, and learning differences than babies born at 39 weeks – not because something is wrong with their brain structure, but because the wiring density is lower.
Every additional week from 35 to 39 meaningfully increases the density of these neural connections. This is the strongest argument for waiting for spontaneous labor in uncomplicated pregnancies.
The Group B Strep Test – What Happens This Week
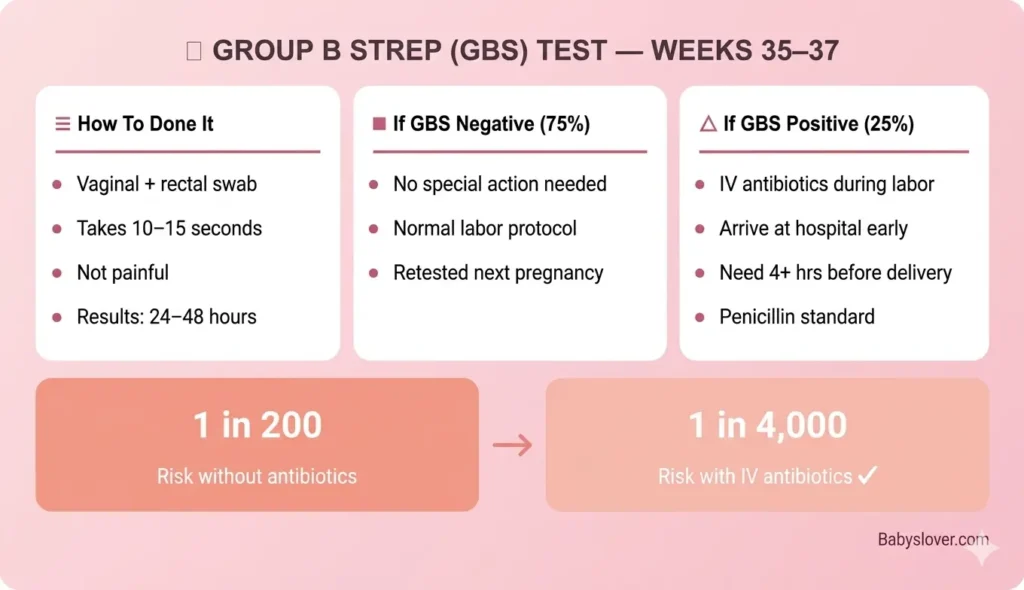
The Group B Streptococcus (GBS) swab test happens at Weeks 35-37 of pregnancy. For many women at 35 weeks pregnant, it will happen at this week’s appointment.
You were introduced to this test at Week 32. Here is the practical reality of what happens:
The procedure:
- Your provider uses a cotton swab to collect samples from your vaginal area and rectum
- The swab takes approximately 10-15 seconds – it is not painful
- The sample is sent to a lab and results return in 24-48 hours
- Your provider contacts you with results – or tells you at your next appointment
| Result | What It Means | What Happens Next |
| GBS Negative | No GBS bacteria detected | No special action needed during labor |
| GBS Positive | GBS bacteria present – approximately 25% of healthy women | IV antibiotics during labor – reduces transmission risk from ~1 in 200 to ~1 in 4,000 |
| Unknown / Not Tested | Test not done or results unavailable at delivery | Provider treats as positive – gives antibiotics as precaution |
If you test GBS positive – key practical points:
- Arrive at the hospital earlier than you might otherwise – you need at least 4 hours of IV antibiotics before delivery for full protection
- The antibiotics are standard penicillin for most women – if you have a penicillin allergy, tell your provider now so an alternative can be planned
- GBS positive status does not change your birth plan in any other way
- GBS status changes between pregnancies – it is tested every pregnancy
- A planned cesarean section with intact membranes does not require GBS antibiotic prophylaxis – discuss this with your provider if relevant
The Mucus Plug – What It Is and What Losing It Means
The mucus plug is a collection of thick cervical mucus that has sealed the cervix since early pregnancy – acting as a physical barrier between the uterus and the outside world. As your cervix begins to soften and efface in preparation for labor, the plug can dislodge and pass.
At 35 weeks pregnant, you may or may not have lost your mucus plug yet. Losing it at this stage does not mean labor is imminent – but it is worth knowing what it looks like and what it signals.
| What It Looks Like | What It Means | When to Call |
| Thick, jelly-like discharge – clear, pink, brown, or blood-tinged – the size of about a teaspoon to tablespoon | Cervix is beginning to soften and open – normal preparation for labor | No need to call immediately unless combined with contractions or heavy bleeding |
| Gradual increase in thick discharge over several days | The plug is releasing gradually – more common than a single event | Mention at your next appointment unless symptoms develop |
| Heavy bright red bleeding with the mucus | Bloody show OR something requiring evaluation | Call your provider – bright red blood warrants assessment |
| No noticeable plug at all | Normal – many women never notice losing it | No action needed |
Losing the mucus plug can happen anywhere from 2 weeks before labor to the morning of labor itself. It is a sign of cervical progress, not a reliable indicator of timing. Some women who lose the plug at 35 weeks pregnant go on to deliver at 40 weeks. Others deliver within days.
The mucus plug can also partially regenerate if not followed quickly by labor – the cervix continues producing mucus even after the original plug passes.
35 Weeks Pregnant Symptoms
Increased Pressure and Pelvic Heaviness
As your baby settles deeper into the pelvis – either already or in the coming weeks – the pressure on your pelvic floor increases substantially. The sensation of carrying something very heavy low in your body, or feeling like the baby is sitting directly on your pelvis, is entirely normal at 35 weeks pregnant.
This pressure tends to worsen with prolonged standing, walking, and by the end of the day. Short rests with your feet elevated, a pregnancy support belt, and pelvic floor exercises (Kegels) all help manage it. The pressure eases after delivery with remarkable speed for most women.
Fatigue at Its Most Intense
The third trimester fatigue that set in around Week 28 has had seven weeks to compound. At 35 weeks pregnant, fatigue is near its peak for most women – driven by the combination of disrupted sleep, increased metabolic demand, physical discomfort, and the sheer effort of carrying a 5+ pound baby through every daily task.
Rest is not laziness at this stage. Your body is doing extraordinary work. Short naps (20-30 minutes), accepting help with physical tasks, and eliminating nonessential commitments are appropriate responses – not indulgences.
Braxton Hicks More Intense and Frequent
By Week 35, Braxton Hicks contractions can be strong enough to stop you mid-sentence. They remain irregular, front-focused, and responsive to hydration and position change – but their intensity has increased as the uterine muscle strengthens in preparation for labor.
The rule remains: if contractions become regular (coming every 10 minutes or more frequently), grow stronger rather than easing, wrap from back to front, or are accompanied by bleeding or fluid, call your provider. At 35 weeks, you are early term – your provider will want to evaluate any pattern that might represent true labor.
Difficulty Breathing
Your diaphragm remains compressed. Climbing stairs, carrying anything heavy, or simply talking for an extended period can leave you breathless. This is normal – and for most women, it improves in the final weeks as the baby descends deeper into the pelvis.
If shortness of breath is sudden, severe, or comes with chest pain or heart palpitations, contact your provider immediately.
Frequent Urination – Every 30 Minutes
Your bladder has almost no capacity at 35 weeks pregnant. Your baby’s head may be resting directly on it. The urge to urinate can arrive with almost no warning and leave you feeling like you never fully emptied. This is the reality of the final weeks – and it intensifies further after the baby drops.
Staying hydrated is still essential, despite the inconvenience. Do not reduce water intake to manage bathroom trips – dehydration compounds fatigue, can trigger Braxton Hicks, and affects amniotic fluid volume.
Late Preterm Birth – What 35 Weeks Actually Means
Babies born between 34 and 36 weeks are classified as late preterm. This is important to understand because late preterm births look healthy to the eye – these babies are close to full size, often breathing independently, and appear robust. But the data tells a different story.
| Risk Factor | Late Preterm (34-36 wks) | Full Term (39-40 wks) | Why the Difference |
| Feeding difficulties | Significantly higher – immature suck-swallow coordination | Low | Feeding reflex not fully coordinated until ~37-38 weeks |
| Temperature regulation | Higher risk of hypothermia | Low | Brown fat deposits incomplete – fat peaks Week 35-38 |
| Jaundice requiring treatment | 2-3x more common | Baseline | Liver enzyme systems not fully mature |
| Respiratory issues | Higher – surfactant near but not at full maturity | Low | Lung maturation completes Week 36-37 |
| Hospital readmission | 3x higher in first month | Baseline | Multiple immature systems contributing |
| Learning differences at school age | Small but measurable increase | Baseline | Brain connectivity phase incomplete |
This is not meant to cause alarm if you are 35 weeks pregnant. The vast majority of babies born at this stage do well and have no lasting complications. The data simply reinforces why, in uncomplicated pregnancies, waiting for spontaneous labor at or near 39-40 weeks produces the best outcomes.
Only about 7% of all live births happen at 35-36 weeks. The overwhelming probability is that you and your baby will have several more weeks together before labor begins.
Nutrition at 35 Weeks Pregnant
| Nutrient | Why It Matters at Week 35 | Daily Target and Sources |
| Protein | Baby gaining 8-12 oz/week – almost entirely fat and muscle. You need ~71g/day minimum. | Chicken, eggs (~6g each), Greek yogurt (~18g/cup), lentils, cottage cheese |
| Healthy fats | Fat deposits at shoulders, cheeks, and limbs are the primary developmental focus this week – dietary fat directly supports this | Avocado, olive oil, nuts, fatty fish, eggs |
| Iron | Blood volume at peak – deficiency causes severe fatigue + impairs oxygen to baby | Red meat, lentils, spinach + vitamin C; supplement if provider recommends |
| DHA (Omega-3) | Brain connectivity phase – synaptogenesis and myelination both require DHA | Salmon, sardines, eggs, prenatal vitamins with DHA |
| Calcium | Bone hardening ongoing – adequate intake protects your bone density | Dairy, fortified milks, sardines with bones, almonds |
| Fiber + Water | Constipation at its worst – hemorrhoid prevention critical | Prunes, oats, beans, vegetables + minimum 8-10 glasses water daily |
Appetite continues to be compressed. High-protein, healthy-fat snacks – avocado toast, Greek yogurt with nuts, eggs with whole grain toast – are more effective than attempting large meals. If nausea has returned in late pregnancy (it does for some women), small cool snacks like fruit, crackers, or smoothies tolerate better than hot heavy meals.
Partner Tips for Week 35
- The GBS test results will come back this week – make sure both of you know what a positive result means and what it requires (earlier hospital arrival, IV antibiotics). No panic needed – just preparation.
- Weekly appointments begin now – if possible, come to at least one of the final appointments. The conversations at Week 36, 37, 38 will include labor signs, position confirmation, and delivery planning.
- The fatigue at Week 35 is real and cumulative – not a mood or an excuse. The most helpful thing you can do is take tasks off her list without being asked.
- If she mentions losing what looks like a mucus plug, note the date and time. It doesn’t mean labor is imminent – but it is worth tracking.
- Make sure the car seat is installed, inspected, and confirmed. The baby could arrive within 5 weeks – or sooner.
- Hospital bag confirmed, route known, care for older children or pets arranged if applicable.
- Ask how she is doing emotionally. The final weeks carry a combination of anticipation, exhaustion, fear, and excitement that can be hard to name – just asking opens space for it.
35 Weeks Pregnant Checklist

| Task | Priority |
| GBS test – confirm it’s done or booked this week | URGENT – do this week |
| Shift to weekly appointments from here until delivery | This week |
| Know what GBS positive result means – share with partner | This week |
| Hospital bag fully packed + by the door + route confirmed | URGENT |
| Continue kick counts daily – 10 in 2 hours | Daily |
| Know mucus plug appearance and what it signals | Awareness |
| Continue perineal massage 1-2x per week if started at Week 34 | Weekly |
| Confirm car seat installed and inspected | This week |
| Birth plan – confirmed, printed, in hospital bag | Confirm this week |
| Cord blood banking decision – final window | This week if undecided |
| Increase healthy fats at meals – avocado, olive oil, nuts, eggs | Daily |
| Iron + vitamin C at meals | Daily |
| DHA prenatal vitamins | Daily |
| Kegel exercises – 3 sets of 10 | Daily |
| Short rest with feet elevated – at least once daily | Daily |
Frequently Asked Questions – 35 Weeks Pregnant
What trimester is 35 weeks pregnant?
35 weeks pregnant is the eighth week of the third trimester. Third trimester runs from Week 28 through Week 40. You have approximately 5 weeks remaining until your due date.
How many months is 35 weeks pregnant?
At 35 weeks pregnant, you are at the end of your eighth month of pregnancy – nearly 9 months. Full-term pregnancy is 40 weeks, which spans approximately 9.5 calendar months. Most people reach their due date between 9 and 10 calendar months from their last period.
How much does a baby weigh at 35 weeks pregnant?
At 35 weeks pregnant, your baby weighs approximately 2.4 to 2.6 kg (about 5.3 to 5.7 lbs) and measures around 46-47 cm from head to heel – roughly the size of a large honeydew melon. This week marks the beginning of the most rapid weight gain phase, with baby gaining 8-12 oz (226-340g) per week from now until birth.
Can a baby survive at 35 weeks?
Yes. Survival rates for babies born at 35 weeks with appropriate NICU support are very high – approximately 97-99%. Most 35-weekers breathe independently or with minimal assistance. They do, however, have higher rates of feeding difficulties, jaundice, and temperature regulation challenges compared to full-term babies, which is why NICU monitoring is standard and why every additional week matters.
What is the GBS test at 35 weeks pregnant?
The Group B Streptococcus (GBS) test is a simple swab of the vaginal area and rectum that checks for GBS bacteria. It typically happens between Weeks 35 and 37. Approximately 25% of healthy women carry GBS with no symptoms. If positive, IV antibiotics are given during labor, reducing the risk of transmission to the baby from approximately 1 in 200 to roughly 1 in 4,000. GBS status changes between pregnancies – it is tested every time.
What does losing the mucus plug look like at 35 weeks?
The mucus plug looks like a thick, jelly-like discharge – typically clear, pink, brown, or lightly blood-tinged – about the size of a teaspoon to tablespoon. It can release all at once or gradually over several days. Losing it at 35 weeks does not mean labor is imminent – some women lose it weeks before labor begins. No immediate action is needed unless you also have regular contractions, heavy bleeding, or a gush of fluid.
What is late preterm birth and what are the risks?
Late preterm birth refers to births between 34 and 36 weeks. Babies born at this stage are close to full size but carry specific risks compared to full-term babies, including higher rates of feeding difficulties, temperature regulation challenges, jaundice, and respiratory issues. These risks exist because several final developmental phases – including brain connectivity, fat deposits, and lung maturation – complete in the 37-40 week window. Only about 7% of live births happen at 35-36 weeks – the overwhelming majority of pregnancies continue well past this point.
Why does my baby feel less active at 35 weeks?
As your baby grows and space inside the uterus becomes tighter, the nature of movement changes – there is less room for full somersaults and more restriction on large movements. You may feel fewer kicks and more rolls, stretches, and shifts. Importantly, the frequency of movement should not significantly decrease – only the type. If you notice a genuine reduction in your baby’s usual movement pattern, do a kick count (10 movements in 2 hours) and contact your provider if you cannot reach 10.
Looking Ahead: 36 Weeks Pregnant
At 36 weeks pregnant, your baby’s lungs reach full maturity, the skin loses most of its remaining wrinkles as fat fills in, and your provider will begin monitoring cervical changes. Week 36 is also when your provider will discuss your birth preferences and confirm any remaining questions about labor recognition and hospital protocols.
Five weeks. Kidneys complete. Rapid fat phase underway. A brain building its final connections. Keep going.
Follow our pregnancy week by week guide for every development from now to delivery.