

Those three words carry the weight of 39 weeks Pregnant of becoming. Full term. Everything your body has been building toward since a fertilized egg implanted into the lining of your uterus has arrived at the destination those words describe.
Your baby’s brain at this moment is approximately 30 percent larger than it was just four weeks ago. Thirty percent. In 4 weeks. The final connectivity phase – the dense web of synaptic links between neurons that were waiting for their partners – is essentially complete. The brain your baby will be born with is ready.
The skin that once let light pass through it is now opaque, thickened, and slightly acidic – a natural pH shift that creates an antimicrobial barrier from the moment of birth. The lungs have enough surfactant to take their first breath, hold it, and breathe again. The eyes are fully connected to the brain. The digestive system is queued and waiting. Everything that needed to be built has been built.
Within the next one to two weeks – perhaps in the next few hours – you will meet the person you have been carrying.
One week from your due date. Here is everything happening at 39 weeks pregnant.

Contents
- 1 Quick Summary: 39 Weeks Pregnant
- 2 What’s Happening in Your Body at 39 Weeks Pregnant
- 3 Baby Development at 39 Weeks Pregnant
- 4 The Skin’s Acid Mantle – Why Delayed Bathing Matters
- 5 39 Weeks Pregnant Symptoms
- 6 The ARRIVE Trial – Induction at 39 Weeks
- 7 What Happens at Birth – The First 60 Minutes
- 8 Nutrition in the Final Days of Full Term
- 9 Partner Tips for Week 39
- 10 39 Weeks Pregnant Checklist
- 11 Frequently Asked Questions – 39 Weeks Pregnant
- 11.1 What trimester is 39 weeks pregnant?
- 11.2 How many months is 39 weeks pregnant?
- 11.3 How much does a baby weigh at 39 weeks pregnant?
- 11.4 Is it safe to give birth at 39 weeks?
- 11.5 What is the Apgar score?
- 11.6 What is delayed cord clamping?
- 11.7 What is the breast crawl?
- 11.8 Why should I delay my baby’s first bath?
- 12 Looking Ahead: 40 Weeks Pregnant
Quick Summary: 39 Weeks Pregnant
| Detail | Info |
| Baby size | Mini watermelon – ~50-51 cm, ~3.2-3.6 kg (7-8 lbs) |
| Trimester | Third trimester – Week 12 of T3 |
| Term status | FULL TERM – optimal developmental window |
| Weeks remaining | 1 week to due date (but may be 2+ weeks) |
| Top milestone | Brain 30% larger than 4 weeks ago + skin acidic barrier + full systemic readiness |
| This week’s action | Know the Apgar score + understand induction options + be ready to go |
What’s Happening in Your Body at 39 Weeks Pregnant

At 39 weeks pregnant, the physical experience of late pregnancy has either reached a peak of discomfort you did not previously think possible, or you have found a kind of exhausted acceptance of it. Both are valid. Both are the end of something.
Your cervix is likely efface and may be dilating – or it may still be closed. Neither tells you reliably when labor will begin. What your body is doing is preparing, incrementally, day by day, for the event that is coming.
You may notice a sudden surge of energy – the nesting instinct in its final expression. Or you may feel the opposite: a profound heaviness, a settling, a feeling of waiting that is unlike anything else. Both of these are recognized patterns in the final days of pregnancy.
Weight gain has essentially stopped for most women at this point. Your body is no longer in an expansion phase – it is in a preparation phase.
What to expect at your Week 39 appointment:
- Blood pressure, urine protein, fundal height – final monitoring
- Baby’s heartbeat – confirmed strong
- Baby’s position – almost certainly head-down by now
- Optional cervical exam – effacement and dilation
- Non-stress test if ordered or if post-dates concerns arise
- Discussion of elective induction at 39 weeks – your provider may offer this now
- Plan for what happens if you reach Week 40 and 41 without labor
Baby Development at 39 Weeks Pregnant

At 39 weeks pregnant, your baby measures approximately 50-51 cm from head to heel and weighs around 3.2 to 3.6 kg – roughly the size of a mini watermelon. Both smaller and larger babies are entirely healthy at full term.
| Detail | Measurement |
| Length | ~50-51 cm (about 19.5-20 inches) |
| Weight | ~3.2-3.6 kg (approx. 7-8 lbs) |
| Size comparison | Mini watermelon |
| Head circumference | ~34 cm (BPD ~94 mm – full-term measurement) |
| Term status | FULL TERM |
Key developments at full term:
- Brain 30% larger than four weeks ago: The final synaptogenesis and myelination sprint is essentially complete. Your baby’s brain at Week 39 has the neural connection density needed for birth, the newborn period, and the rapid learning that begins in the first hours of life. The brain that will recognize your face, turn toward your voice, and begin mapping the world starts functioning from the moment your baby is born.
- Skin thickened and acidic: The skin has completed its final transformation. It is now opaque, multi-layered, and has undergone a pH shift – becoming slightly acidic (around pH 5.5). This acidity is not random. It creates what is known as the acid mantle – a natural antimicrobial barrier that provides passive protection against pathogens from the moment of birth. The standard practice of washing newborns immediately removes this protection. This is one of the strongest arguments for delayed newborn bathing.
- Eyes fully connected to brain: The visual pathway from the retina through the optic nerve to the visual cortex is complete. Your baby can detect light and darkness, distinguish high-contrast patterns, and focus clearly at 8-12 inches – the distance to your face during feeding. Full color vision and adult visual acuity will develop over the first 6-12 months after birth.
- Lungs: final surfactant complete: Surfactant production is at term levels. The alveoli – the tiny air sacs in the lungs – can now inflate on the first breath and stay open between breaths. Lung maturation continues after birth and does not complete until around age 8, but the lungs are entirely functional for independent breathing from the moment of birth.
- Liver enzymes mature: The liver’s bilirubin-processing enzymes are at full capacity. This is why the jaundice rate at 39-40 weeks is lower than at 37-38 weeks – the liver can process bilirubin more efficiently. Jaundice still affects some full-term newborns, but with less frequency and severity than in early-term births.
- All reflexes operational: The rooting reflex, sucking reflex, grasp reflex, Moro (startle) reflex, stepping reflex, and tonic neck reflex are all present and testable from birth. These reflexes will be assessed in your baby’s first examination.
- Vernix: mostly reabsorbed: Most of the vernix caseosa has dissolved back into the amniotic fluid as fluid volume has declined. Some vernix may remain in skin creases – at the neck, armpits, and groin. This remaining vernix is protective and beneficial; the WHO recommends leaving it in place and delaying the first bath.
The Skin’s Acid Mantle – Why Delayed Bathing Matters
At 39 weeks, your baby’s skin has undergone a final pH transformation that most parents and even many healthcare providers do not know about.
At birth, a baby’s skin has a pH of approximately 6.5 – neutral. Within hours to days of birth, the skin’s surface acidifies to around pH 5.5, creating what is called the acid mantle. This acidification is driven by the activation of sebaceous glands and by the natural microbiome colonizing the skin surface.
The acid mantle is the skin’s primary antimicrobial defense. At pH 5.5, the skin surface is hostile to the growth of pathogenic bacteria. Staphylococcus aureus, for example, grows poorly below pH 6. The acid mantle also supports the skin’s structural integrity, helps maintain moisture, and promotes the colonization of beneficial commensal bacteria.
Bathing a newborn immediately after birth with alkaline soap removes the vernix, strips the developing acid mantle, and temporarily disrupts this protective system. The World Health Organization recommends delaying the first bath for at least 24 hours – or ideally longer – specifically to protect the acid mantle during its formation.
When you are at the hospital and staff suggest bathing your newborn, you are entirely within your rights to request a delay. This is supported by WHO guidance. Your baby’s skin protection begins at birth – and an immediate bath removes it.
39 Weeks Pregnant Symptoms
Pelvic Pressure: Maximum
At 39 weeks pregnant, your baby’s head is almost certainly engaged deep in the pelvis. The pressure on your pelvic floor, bladder, and lower back is at its maximum. The sensation of something pressing down constantly from inside is not imagined – it is a near-term baby’s head, directly above your cervix.
This pressure is one of the more reliable signs that your body is in its final preparation phase. Walking may help with mild relief as movement encourages the head to settle deeper. Resting with your feet elevated helps with the associated swelling and fatigue.
Contractions – Distinguishing Prodromal from Active Labor
At 39 weeks pregnant, contractions of various types are extremely common. Braxton Hicks can be strong and frequent. Prodromal labor – regular contractions that stop and restart over days without progressing – affects many women in the final weeks.
The question every 39-week pregnant woman is asking is the same one: is this real?
The honest answer is that the only way to know with certainty is to be assessed by your provider. If you are uncertain, call and describe what you are feeling. At 39 weeks, labor assessment is appropriate and expected.
What distinguishes active labor is progression: contractions that become longer, stronger, and closer together over time – and do not stop. The 5-1-1 rule (every 5 minutes, lasting 1 minute, for 1 hour) remains the standard threshold for first-time mothers. Second pregnancies often progress faster – call earlier.
Extreme Fatigue
The fatigue at 39 weeks pregnant is unlike any fatigue earlier in pregnancy. It is the combination of cumulative sleep deprivation, the weight of carrying a full-term baby through every daily movement, the physical demands of a body that is preparing for labor, and the emotional intensity of being this close to the end.
Rest is not only appropriate – it is physiologically important. Sleep deprivation in the final days affects labor duration and pain perception. If you can sleep, sleep. If you cannot sleep, rest horizontally. Your body is conserving energy for something significant.
Emotional Readiness – The Final Shift
Many women at 39 weeks pregnant describe a shift in emotional state that is different from anything they have felt before – a sense of being done being pregnant, a readiness that moves past impatience into something quieter. A feeling of waiting that is not anxious but almost expectant in a physical sense.
This emotional shift is not just psychological. Research suggests the same hormonal changes that prepare the body for labor also produce neurological changes that increase maternal readiness and reduce the fear response. Your brain is preparing you in parallel with your body.
Whatever you are feeling right now – terrified, ready, numb, overwhelmed, excited, all of the above – is appropriate. There is no wrong way to feel at 39 weeks pregnant.
The ARRIVE Trial – Induction at 39 Weeks
In 2018, a landmark study called the ARRIVE trial (A Randomized Trial of Induction Versus Expectant Management) changed the conversation about labor induction at 39 weeks.
The ARRIVE trial enrolled 6,106 first-time mothers with low-risk pregnancies and randomly assigned them to either elective induction at 39 weeks or expectant management (waiting for spontaneous labor). The results were surprising to many in the obstetric community.
| Outcome | Elective Induction at 39 Weeks | Expectant Management (Waiting) |
| Cesarean section rate | 18.6% – LOWER | 22.2% – HIGHER |
| NICU admission | No significant difference | No significant difference |
| Perinatal death or serious complications | No significant difference | No significant difference |
| Maternal complications | Lower in induction group | Higher in expectant group |
| Stillbirth risk | Slightly lower in induction group | Slightly higher due to placental aging after 40 weeks |
| Time to delivery | Shorter – delivery earlier | Longer – may wait to 41+ weeks |
The ARRIVE trial led ACOG to update its guidance: elective induction at 39 weeks in low-risk, first-time mothers is reasonable to offer and discuss. It does not increase cesarean risk (and may actually reduce it) and carries no increased neonatal risk.
This does not mean induction at 39 weeks is right for everyone – or that waiting is wrong. It means the conversation has changed. If your provider offers to discuss elective induction at this week’s appointment, you now know the study behind that conversation.
Questions to ask your provider:
- Am I a candidate for elective induction based on my cervical status?
- What induction method would be used for my situation?
- What are the specific risks and benefits for my case?
- What is the difference between waiting for spontaneous labor and induction at 39 weeks for me specifically?
What Happens at Birth – The First 60 Minutes
Most pregnancy guides focus almost exclusively on labor and delivery. Very few prepare parents for what actually happens in the room after the baby arrives – the first hour of life. Here is what to expect.
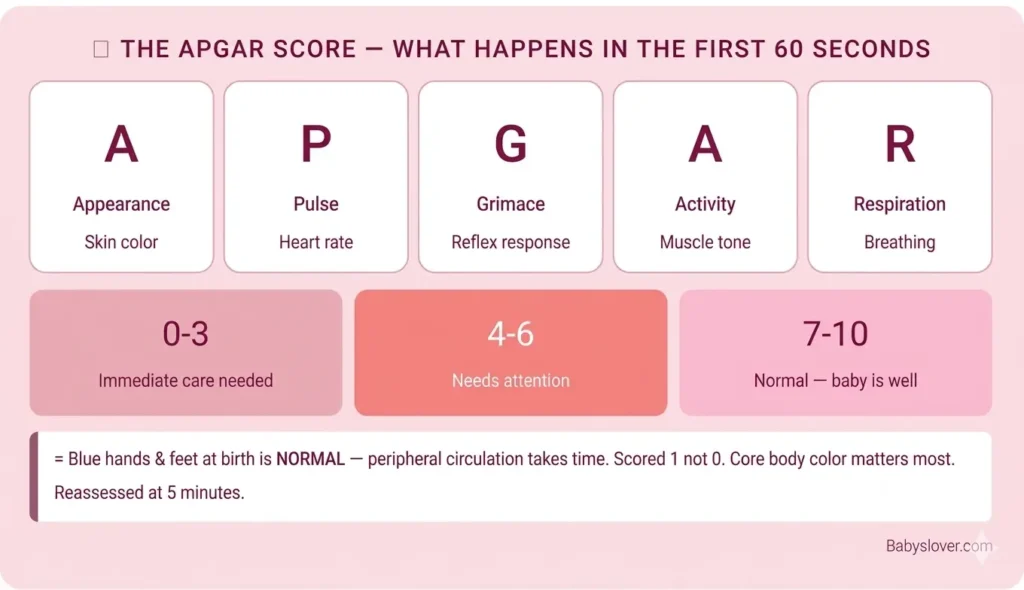
The first 60 seconds – Apgar score:
Within 60 seconds of birth, a nurse or midwife will assess your baby on the Apgar scale – a 10-point score evaluating five signs of newborn health.
| Apgar Sign | 0 points | 1 point | 2 points |
| Appearance (skin color) | Blue or pale all over | Blue hands/feet, pink body | Pink all over |
| Pulse (heart rate) | Absent | Below 100 bpm | 100+ bpm |
| Grimace (reflex/response) | No response to stimulation | Grimace only | Cry, cough, or sneeze |
| Activity (muscle tone) | Limp | Some limb flexion | Active movement |
| Respiration (breathing) | Absent | Weak, irregular | Strong cry |
| Apgar Score | What It Means | What Typically Happens |
| 7-10 | Normal – baby is well | Standard care, placed on mother’s chest |
| 4-6 | Below normal – needs attention | Stimulation, supplemental oxygen if needed |
| 0-3 | Requires immediate intervention | Resuscitation team response |
The Apgar is reassessed at 5 minutes. Most babies score 7-10 and need no intervention. Blue hands and feet at birth (which gives a 1 rather than 2 on Appearance) is normal – peripheral circulation takes time to establish. The core of your baby’s body will be pink even if the extremities are blue.
Babies are not born screaming. It takes several seconds for most babies to clear their airways, take a breath, and cry. This is normal. The first cry may be a single shout – not the sustained wailing of films. Your provider and nurses are watching carefully in these seconds.
Delayed cord clamping:
The umbilical cord continues pulsing for 1-5 minutes after birth, delivering an additional 80-100 mL of placental blood to your baby. This blood is rich in iron and stem cells. The WHO and ACOG both recommend waiting at least 30-60 seconds before clamping – and many providers now wait until the cord has stopped pulsing entirely.
If cord blood banking is part of your plan, this needs to be coordinated with your provider in advance – delayed cord clamping and cord blood collection can sometimes be combined, but the timing and protocol require advance planning.
The newborn exam:
Within the first hour (sometimes in the delivery room, sometimes in the nursery depending on your hospital), your baby will receive:
- Vitamin K injection: Newborns are born with very low Vitamin K – the clotting factor that prevents dangerous bleeding. A single intramuscular injection within hours of birth prevents a rare but serious condition called Vitamin K Deficiency Bleeding (VKDB)). The AAP strongly recommends this for all newborns.
- Eye prophylaxis: Erythromycin ointment applied to the eyes prevents gonorrheal eye infection that can occur during vaginal birth. Some hospitals still do this routinely; practice varies by state and country.
- Hepatitis B vaccine: The first dose is typically given within 24 hours of birth.
- Newborn screening: A heel prick blood test screens for dozens of metabolic conditions, including PKU, hypothyroidism, and sickle cell disease. The specific panel varies by state.
- Hearing screen: Before discharge, a hearing test using soft sounds and sensors checks for hearing loss.
Skin-to-skin contact and the breast crawl:
If you and your baby are both stable, skin-to-skin contact begins immediately after birth. Your baby is placed directly on your chest, both of you covered with a warm blanket.
What happens next, when allowed to unfold naturally, is remarkable. Most newborns placed skin-to-skin within 30 minutes of birth will, given time, locate the breast and begin to feed – a sequence called the breast crawl. The mechanism driving it is primarily olfactory: the Montgomery glands on your areola produce a secretion that smells similar to amniotic fluid, which your baby’s olfactory system recognizes from prenatal exposure. Your newborn navigates toward that familiar scent.
Skin-to-skin also stabilizes your baby’s heart rate, temperature, and blood sugar – measurably better than an incubator in healthy newborns. It initiates bonding hormones in both you and your baby. And it is the single best start to breastfeeding if that is your intention.
Nutrition in the Final Days of Full Term
| Nutrient | Why It Still Matters at Week 39 | Best Sources |
| Iron | Postpartum hemorrhage + recovery + breast milk iron all depend on your iron stores built NOW | Red meat, lentils, spinach always paired with vitamin C |
| Protein | Birth recovery – vaginal tearing or cesarean incision both require protein to heal. Milk production begins within days. | Chicken, eggs, Greek yogurt, lentils, cottage cheese |
| Healthy fats | Breast milk is 50% fat – your dietary fat composition directly influences the first milk your baby receives | Avocado, olive oil, nuts, fatty fish, full-fat dairy |
| DHA (Omega-3) | Your DHA transfers directly into breast milk. Baby’s brain development continues post-birth and requires DHA. | Salmon, sardines, eggs, prenatal vitamins with DHA |
| Fiber + Water | Post-birth constipation is nearly universal – especially after cesarean. Building gut health now helps. | Prunes, oats, beans, water at least 8-10 glasses daily |
| Calcium | Breastfeeding pulls calcium from your bones if dietary intake is insufficient – begins immediately after birth | Dairy, fortified plant milks, sardines, almonds |
Eat what you can, when you can. Your appetite at 39 weeks may be unpredictable. Prioritize iron, protein, and DHA specifically – these are the nutrients that will matter most in the first weeks after birth.
Partner Tips for Week 39
- The ARRIVE trial – read at least the summary. If your provider offers to discuss elective induction, you need to be part of that informed conversation.
- Know the Apgar score. When the nurse calls out numbers at one minute and five minutes after birth, you will know what they mean. This reduces anxiety and keeps you present rather than confused.
- Know delayed cord clamping – ask for it explicitly if it is not automatically offered, especially if you have chosen not to do cord blood banking.
- Advocate for delayed bathing if immediate bath is standard in your hospital. Say ‘We would like to delay the first bath’ – this is supported by WHO guidance and most staff will accommodate it.
- Know what the first 60 minutes will look like – the Apgar assessments, the Vitamin K injection, the newborn exam. Being prepared means you can be present with your baby rather than anxiously watching unfamiliar procedures.
- The labor that begins at 39 weeks may take hours. Sustain yourself – eat before you go to the hospital, bring food, rest during the early phase if possible. You are support staff for this event, and your endurance matters.
- After the baby is born and the room quiets: say nothing. Just be there. The first moments are complete in themselves.
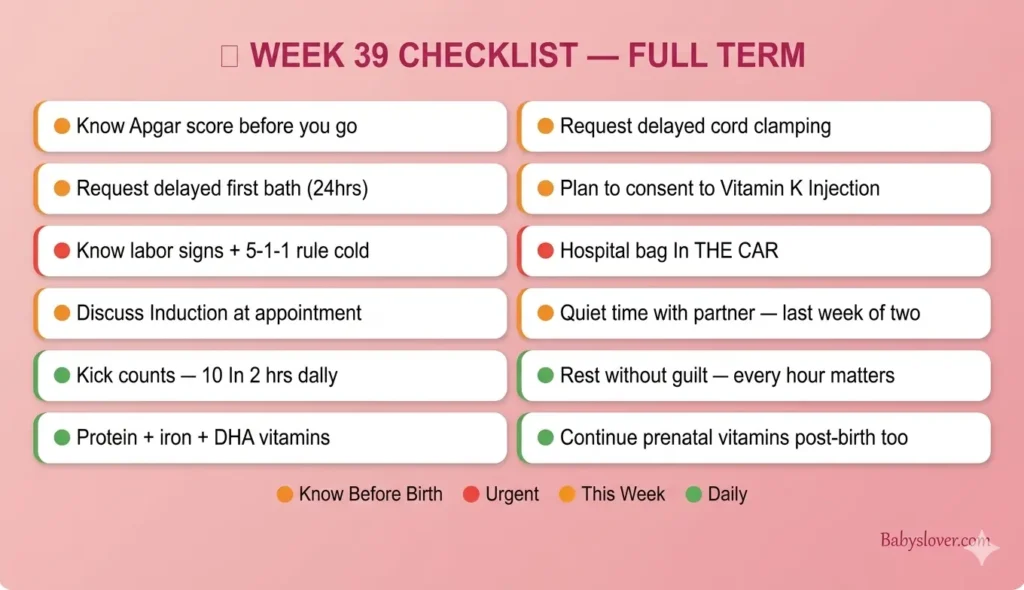
39 Weeks Pregnant Checklist
| Task | Priority |
| Know labor signs + 5-1-1 rule + when to call – know these cold | URGENT |
| Hospital bag in the car – confirmed one final time | URGENT |
| Know hospital directions + overnight entrance + where to park | URGENT |
| Discuss elective induction at this week’s appointment if curious | This week |
| Know the Apgar score and what the numbers mean | Know this now |
| Know delayed cord clamping – ask for it explicitly | Know before you go |
| Know delayed bathing – request it at the hospital | Know before you go |
| Understand Vitamin K injection – plan to consent | Know before you go |
| Continue kick counts – 10 in 2 hours, every day | Daily |
| Rest without guilt – every hour of sleep now matters | Daily priority |
| Protein + iron + healthy fats at every meal | Daily |
| DHA prenatal vitamins – continue through birth and postpartum | Daily |
| GBS result known + hospital timing if positive confirmed | Confirm now |
| Birth plan in hospital bag – partner has read it | Confirm now |
| Newborn care items confirmed – safe sleep setup, car seat installed | Confirm this week |
| Spend quiet time with your partner – this is the last week of two | This week |
Follow our pregnancy week by week guide for every development from now to delivery.
Frequently Asked Questions – 39 Weeks Pregnant
What trimester is 39 weeks pregnant?
39 weeks pregnant is the twelfth week of the third trimester and the beginning of full term. Third trimester runs from Week 28 through Week 40. You have approximately 1 week remaining until your due date – though labor may begin sooner or later.
How many months is 39 weeks pregnant?
At 39 weeks pregnant, you are 9 to 10 months pregnant. Pregnancy spans 40 weeks – approximately 9.5 calendar months. The due date at 40 weeks marks the statistical midpoint, not a deadline. Labor before or after the due date is normal within the 38-42 week window.
How much does a baby weigh at 39 weeks pregnant?
At 39 weeks pregnant, your baby weighs approximately 3.2 to 3.6 kg (about 7 to 8 lbs) and measures around 50-51 cm from head to heel – roughly the size of a mini watermelon. Healthy birth weight varies significantly. Babies smaller or larger than this average range may be entirely healthy, and birth weight is only one of many indicators your provider monitors.
Is it safe to give birth at 39 weeks?
Yes – 39 weeks is full term and the optimal birth window according to ACOG. A baby born at 39 weeks has completed all major developmental phases. The ARRIVE trial found that elective induction at 39 weeks in low-risk first-time mothers did not increase cesarean risk and had no worse neonatal outcomes compared to waiting for spontaneous labor. Every day from 39 to 40 weeks continues to be safe and beneficial.
What is the Apgar score?
The Apgar score is a 10-point newborn assessment given at 1 and 5 minutes after birth. It evaluates five signs: Appearance (skin color), Pulse (heart rate), Grimace (reflex response), Activity (muscle tone), and Respiration. Each is scored 0, 1, or 2. A score of 7-10 is normal and means your baby is doing well. Scores below 7 prompt additional assessment or intervention. Blue hands and feet (scoring 1 for Appearance) is normal at birth – peripheral circulation takes time to establish.
What is delayed cord clamping?
Delayed cord clamping means waiting at least 30-60 seconds (and often until the cord stops pulsing) before cutting the umbilical cord after birth. During this time, the cord continues delivering placental blood to the baby – approximately 80-100 mL additional, rich in iron and stem cells. Both WHO and ACOG recommend delayed cord clamping as standard practice. If you want it, request it explicitly at the hospital.
What is the breast crawl?
The breast crawl is the natural sequence in which a newborn placed skin-to-skin on the mother’s chest will, given time and minimal intervention, locate the breast and initiate feeding. It is driven primarily by the baby’s sense of smell – the Montgomery glands around the areola produce a secretion that smells similar to amniotic fluid, which the newborn’s olfactory system recognizes. Most newborns complete the breast crawl within 30-60 minutes of birth when not interrupted. Allowing this process to unfold supports early breastfeeding success.
Why should I delay my baby’s first bath?
The vernix remaining on a newborn’s skin at birth is protective and has antibacterial properties. The newborn’s skin also undergoes a pH shift after birth, forming an acid mantle – a slightly acidic surface that inhibits pathogenic bacteria. Immediate bathing removes vernix, disrupts the developing acid mantle, can cause temperature instability, and has been associated with lower breastfeeding initiation rates. The WHO recommends delaying the first bath for at least 24 hours. You can request this explicitly at the hospital.
Looking Ahead: 40 Weeks Pregnant
At 40 weeks pregnant, you have reached your due date. Your baby may arrive this week – or may need another few days or weeks. Both are within the normal range of human birth timing. Your provider will discuss monitoring plans and induction timing if labor has not yet begun. The wait that felt like forever is almost over.
One week. A brain 30% larger than it was a month ago. Skin with its own antimicrobial barrier. Eyes connected to the brain and ready to find your face. You have made it to full term. This is what all of it was building toward. For everything from here through delivery, our pregnancy tips for first time moms is with you every step. 💗