

36 Weeks Pregnant, something is forming inside your baby that will be the first thing your newborn passes in the hours after birth.
As your baby swallows amniotic fluid in the final weeks of pregnancy, that fluid carries particles of vernix caseosa and shed lanugo. These accumulate in your baby’s intestines, mixing with bile produced by the liver. The result is meconium – a dark greenish-black, tarry substance that will be your baby’s first bowel movement, typically passed in the first 24 hours of life. Your baby’s digestive system has been quietly building this supply for weeks. The collection is nearly complete.
Your baby’s skull is also doing something this week that will make delivery possible. The six bone plates that make up the skull are still separate and flexible, able to overlap and compress during delivery – a process called molding. When your newborn arrives with a slightly pointed or asymmetrical head, this is why. The skull returns to its rounded shape within hours to days.
And if you have been told you are 36 weeks pregnant and feeling impatient, there is something important to understand about what 36 weeks means – and what it does not.
Four weeks from your due date. Here is everything happening at 36 weeks pregnant.

Contents
- 1 Quick Summary: 36 Weeks Pregnant
- 2 What’s Happening in Your Body at 36 Weeks Pregnant
- 3 Baby Development at 36 Weeks Pregnant
- 4 36 Weeks Is NOT Full Term – Why This Matters
- 5 Meconium – What It Is and Why It’s Forming Right Now
- 6 Skull Molding – The Mechanics Behind a Pointy Head at Birth
- 7 36 Weeks Pregnant Symptoms
- 8 ECV – External Cephalic Version for Breech Babies
- 9 True Labor vs. False Labor – The Definitive Guide for Week 36
- 10 Nutrition at 36 Weeks Pregnant
- 11 Partner Tips for Week 36
- 12 36 Weeks Pregnant Checklist
- 13 Frequently Asked Questions – 36 Weeks Pregnant
- 13.1 What trimester is 36 weeks pregnant?
- 13.2 How many months is 36 weeks pregnant?
- 13.3 How much does a baby weigh at 36 weeks pregnant?
- 13.4 Is 36 weeks full term?
- 13.5 What is ECV for a breech baby at 36 weeks?
- 13.6 How do I know if I’m in labor at 36 weeks?
- 13.7 What is meconium and when does my baby pass it?
- 13.8 Why does my baby’s head look pointed at birth?
- 14 Looking Ahead: 37 Weeks Pregnant
Quick Summary: 36 Weeks Pregnant
| Detail | Info |
| Baby size | Romaine lettuce / large papaya – ~47-48 cm, ~2.6-2.9 kg (5.7-6.4 lbs) |
| Trimester | Third trimester – Week 9 of T3 |
| Months pregnant | 9 months pregnant |
| Weeks remaining | 4 weeks to due date (but full term is Week 39) |
| Top milestone | Skull molding ready for birth + meconium forming + digestion complete |
| This week’s action | Internal cervical exam + ECV if baby is breech + know labor signs |
What’s Happening in Your Body at 36 Weeks Pregnant

At 36 weeks pregnant, your uterus has reached its maximum height – pressing against your ribcage, stomach, lungs, and liver simultaneously. If your baby has engaged in the pelvis, you may have already noticed some welcome relief – a sense of being able to breathe more deeply, heartburn easing, and your bump sitting slightly lower. This is called lightening, and it comes with a trade: better breathing, but increased pelvic pressure, more frequent urination, and more intense lightning crotch episodes.
Weekly appointments are now standard from this point until delivery. At each visit, your provider will monitor blood pressure, urine protein, fundal height, baby’s heartbeat, and baby’s position. Starting around Week 36, many providers also offer an internal cervical exam to check for effacement (thinning) and dilation (opening) of the cervix. This exam is optional – you can decline – and a finding of 0 cm dilation or 0% effacement at Week 36 tells you nothing definitive about when labor will begin.
What to expect at your Week 36 appointment:
- Blood pressure, urine protein, fundal height – standard checks
- Baby’s position – this is the week ECV would be offered if baby is still breech
- GBS results if test was done last week
- Optional internal cervical exam – effacement and dilation
- Discussion of labor signs and when to go to the hospital
- Hospital bag and logistics confirmation
- Any remaining birth plan questions
Baby Development at 36 Weeks Pregnant
IMAGE 2 HERE – Baby development card: baby-development-36-weeks-pregnant.jpg (800×900 px)
At 36 weeks pregnant, your baby measures approximately 47-48 cm from head to heel and weighs around 2.6 to 2.9 kg – roughly the size and weight of a large romaine lettuce or papaya.
| Detail | Measurement |
| Length | ~47-48 cm (about 18.5-19 inches) |
| Weight | ~2.6-2.9 kg (approx. 5.7-6.4 lbs) |
| Size comparison | Romaine lettuce / large papaya |
| Heart rate | 110-160 bpm |
| Skull status | Plates separate, flexible, ready for molding during delivery |
Key developments this week:
- Skull ready for molding: The six bone plates of the skull remain separate and flexible – held together by fibrous seams called sutures. During delivery, these plates can overlap and compress, temporarily reducing the skull’s circumference by up to 1 cm. This is called molding, and it is the reason vaginal delivery is possible at all. The process is entirely normal. The head returns to its rounded shape within hours.
- Meconium almost complete: Your baby’s intestines have been collecting swallowed amniotic fluid, vernix, and lanugo for weeks. This material, mixed with bile, forms meconium – the dark, tarry first bowel movement. It is nearly fully accumulated now and waiting for the stimulation of birth to trigger release.
- Digestion fully ready: The suck-swallow-digest coordination is complete. Your baby can receive colostrum from the first feeding and process it through an entirely functional digestive system. Liver enzymes, pancreatic enzymes, stomach acid production – all assembled and waiting.
- Skin smooth and plump: The skin has lost almost all its wrinkles as fat has filled in underneath. The once-translucent skin of earlier weeks is now opaque, smooth, and soft. Your baby’s appearance is approaching the rounded, soft look of a full-term newborn.
- Fat deposits nearly complete: The fat at the cheeks, shoulders, thighs, and upper arms continues accumulating. A 36-week baby has approximately 15% body fat – compared to roughly 2-3% at 28 weeks. This fat is both insulation and energy reserve.
- Lungs at near-full maturity: Surfactant production is at near-term levels. The lungs are ready to take their first breath. A baby born at 36 weeks today would very likely breathe independently without assistance.
- Circulation and immune systems ready: Cardiac function is fully developed. The placental antibody transfer that has been ongoing since Week 28 is reaching its final phase – your baby is carrying its maximum load of maternal immunity at birth.
36 Weeks Is NOT Full Term – Why This Matters
This is one of the most important things to understand at 36 weeks pregnant – and one of the least clearly explained in most pregnancy resources.
The American College of Obstetricians and Gynecologists (ACOG) classifies pregnancy timing as follows:
| Classification | Weeks | What It Means |
| Preterm | Before 37 weeks | Baby is early – organs, brain, and fat deposits may be incomplete |
| Early Term | 37 weeks 0 days to 38 weeks 6 days | Baby is developed but final brain connectivity and fat phases are still ongoing |
| Full Term | 39 weeks 0 days to 40 weeks 6 days | Optimal developmental completion – recommended window for planned deliveries |
| Late Term | 41 weeks 0 days to 41 weeks 6 days | Post-dates – monitoring intensifies |
| Post Term | 42 weeks and beyond | Placenta aging – induction typically recommended |
At 36 weeks pregnant, you are in the final days of the preterm window. Week 37 is early term – still not full term. Week 39 is full term.
Why does this matter? Because the difference between 36 weeks and 39 weeks includes three full weeks of brain connectivity development (the synaptogenesis and myelination phase), the final stage of fat accumulation, and the completion of liver enzyme maturation. Babies born at 36 weeks versus 39 weeks show measurable differences in feeding success, temperature regulation, and neurodevelopmental outcomes in the first months of life.
This is not a reason for anxiety at 36 weeks – the vast majority of pregnancies reach 39 weeks or beyond. It is, however, a reason to understand why providers do not recommend elective delivery before 39 weeks in uncomplicated pregnancies, and why the phrase ‘basically full term’ at 36 weeks is technically inaccurate.
Meconium – What It Is and Why It’s Forming Right Now
Almost every pregnancy guide mentions that newborns pass a dark, tarry first stool called meconium. Almost none explain where it comes from or how it accumulates during pregnancy. Here is the full story.
From around Week 20 onward, your baby swallows amniotic fluid. That fluid is not sterile – it contains shed skin cells, lanugo, and particles of vernix caseosa. These materials pass into the baby’s developing digestive system and accumulate in the small and large intestines.
At the same time, the liver has been producing bile since around Week 12. Bile flows into the intestines continuously, mixing with the accumulated material. The result is meconium – a combination of intestinal epithelial cells, lanugo, vernix, bile, and amniotic fluid that has been slowly building for months.
By 36 weeks pregnant, the meconium supply is nearly complete. At birth, the sensory and neurological stimulation of delivery triggers peristalsis – the intestinal contractions that move contents through the bowel – and meconium is typically passed within the first 24-48 hours.
| Question | Answer |
| When is meconium passed? | Usually within 24 hours of birth – the AAP recommends concern if it hasn’t passed by 48 hours |
| What does it look like? | Dark greenish-black, thick and tarry – unlike any subsequent bowel movement |
| Is it normal to be worried by the color? | It is normal to be surprised – but meconium is completely normal and expected |
| What about meconium in the amniotic fluid? | If meconium is passed before birth (in utero), it turns the amniotic fluid greenish – this is called meconium-stained fluid and requires evaluation at delivery |
| After meconium comes transitional stool | Days 2-4 bring greenish-brown transitional stool as milk intake begins. By Days 4-5, stool reflects whether baby is breastfed (yellow, seedy) or formula-fed (tan, pasty) |
Skull Molding – The Mechanics Behind a Pointy Head at Birth
Your baby’s skull at 36 weeks pregnant consists of six separate bone plates – the two frontal bones, two parietal bones, the occipital bone at the back, and the temporal bones at the sides. These plates are not yet fused. They are held in position by flexible fibrous seams called sutures and meet at the fontanelles – the soft spots you will feel on your newborn’s head.
During delivery, as the head passes through the narrowest point of the birth canal, the skull plates can shift, overlap, and compress – temporarily reducing the circumference of the skull by up to 1 cm. This process is called molding.
The result of molding is the characteristic cone-head appearance that many newborns have at birth – particularly those born after a long or difficult labor, or after vacuum or forceps assistance. Parents are often startled by this. It is completely normal and completely temporary. The skull plates spring back to their natural positions over the hours and days following delivery.
Babies born by planned cesarean section without labor typically do not show molding – their heads are rounder at birth because the skull plates were not compressed.
Molding is not painful for your baby and does not cause brain injury. The brain is protected by cerebrospinal fluid inside the skull, which buffers the compression. The process has been refined by millions of years of evolution specifically to make large-brained babies passable through a human pelvis.
36 Weeks Pregnant Symptoms
Engagement and Lightening
If your baby has dropped into the pelvis – a process that happens earlier for first-time mothers and often not until labor for subsequent pregnancies – you will notice distinct changes in how your body feels.
| Before Engagement | After Engagement (Lightening) |
| Pressure high in abdomen / on diaphragm | Pressure moves low – pelvis feels full and heavy |
| Heartburn frequent and intense | Heartburn may ease noticeably |
| Shortness of breath with normal activity | Breathing feels easier – more lung room |
| Bladder feels crowded but not direct pressure | Baby’s head directly on bladder – urgency is immediate and constant |
| Bump sits high and round | Bump appears to have moved lower – ‘dropped’ |
Lightening does not mean labor is imminent – in first-time mothers it commonly happens 2-4 weeks before labor. If this is not your first pregnancy, your baby may not engage until labor begins. Both patterns are normal.
Cervical Changes – Effacement and Dilation
At your Week 36 appointment, your provider may offer an internal exam to check cervical progress. Here is what those numbers and percentages mean:
| Term | What It Measures | What Is Normal at Week 36 |
| Effacement (%) | How much the cervix has thinned. 0% = thick and long. 100% = paper thin. | Anywhere from 0-100% – all are normal. Effacement can begin weeks before labor. |
| Dilation (cm) | How open the cervix is. 0 cm = closed. 10 cm = fully dilated for pushing. | Anywhere from 0-3 cm before labor begins. 0 cm does not mean labor won’t start soon. |
| Station | Where the baby’s head is relative to the ischial spines. -3 to +3 scale. | Negative numbers = above the spines. 0 = at the spines. Positive = below (engaged). |
| Cervical position | Where the cervix sits – posterior (back) vs anterior (forward) | Moving from posterior to anterior is a sign of cervical ripening for labor |
Important: cervical exam findings at 36 weeks do not reliably predict when labor will begin. A woman with 3 cm dilation and 80% effacement may labor in two weeks. A woman at 0 cm and 0% effacement may go into labor the next day. The cervix is not a countdown timer.
The exam is optional and can be declined. It carries a tiny risk of inadvertently stimulating contractions or rupturing membranes in rare cases. Ask your provider what information they expect to gain from the exam before agreeing.
Increased Mucus and Discharge
Vaginal discharge increases significantly at 36 weeks as your cervix softens and produces more mucus. You may notice thicker, heavier discharge on a daily basis – this is leukorrhea and is completely normal.
The distinction to remain aware of: watery, colorless, continuous discharge that does not stop may be amniotic fluid. Put on a clean pad and rest for 30 minutes. If the pad is wet when you stand, contact your provider. At 36 weeks, ruptured membranes require evaluation – your baby is ready, but your provider will want to confirm position, GBS status, and monitor for infection.
Intense Braxton Hicks
By 36 weeks, Braxton Hicks can be strong enough to cause you to stop mid-activity and breathe through them. Many women at this stage make a trip to the hospital only to be sent home when contractions turn irregular and subside.
This is not a failure of judgment – it is an extremely common experience, and hospitals and providers expect it. When in doubt, go in. The only way to confirm whether you are in labor is to be assessed.
ECV – External Cephalic Version for Breech Babies
If your baby is still in a breech position (bottom or feet toward the cervix) at Week 36, your provider will likely discuss External Cephalic Version (ECV) – a procedure to manually turn the baby from outside the abdomen.
ECV is typically performed at 36-37 weeks, in a hospital setting where the baby can be monitored.
| Question | Answer |
| How does it work? | Provider places hands on the abdomen and applies firm, steady pressure to guide the baby into a head-down position – usually taking 5-15 minutes |
| Success rate? | Approximately 50-65% of attempts are successful. Higher success rates in subsequent pregnancies and with more experienced providers. |
| Is it painful? | Uncomfortable – some women find it mildly painful. Medication can be given to relax the uterus beforehand. |
| Risks? | Low risk overall – approximately 1% chance of placental abruption or need for emergency delivery. Always performed in a hospital setting for this reason. |
| What if it fails? | Cesarean section is the most common recommendation for term breech presentation. Vaginal breech birth is possible in some settings with experienced providers. |
| Should I try it? | Discuss with your provider – your individual anatomy, placenta position, and other factors affect both the likelihood of success and the risk profile |
About 96-97% of babies are head-down by the time of delivery. If ECV is successful, your birth plan remains largely unchanged. If it is not successful or you decline, your provider will discuss your delivery options.
True Labor vs. False Labor – The Definitive Guide for Week 36
The single most-searched question at 36 weeks pregnant is some variation of ‘how do I know if I’m in labor.’ Here is the most complete answer available.
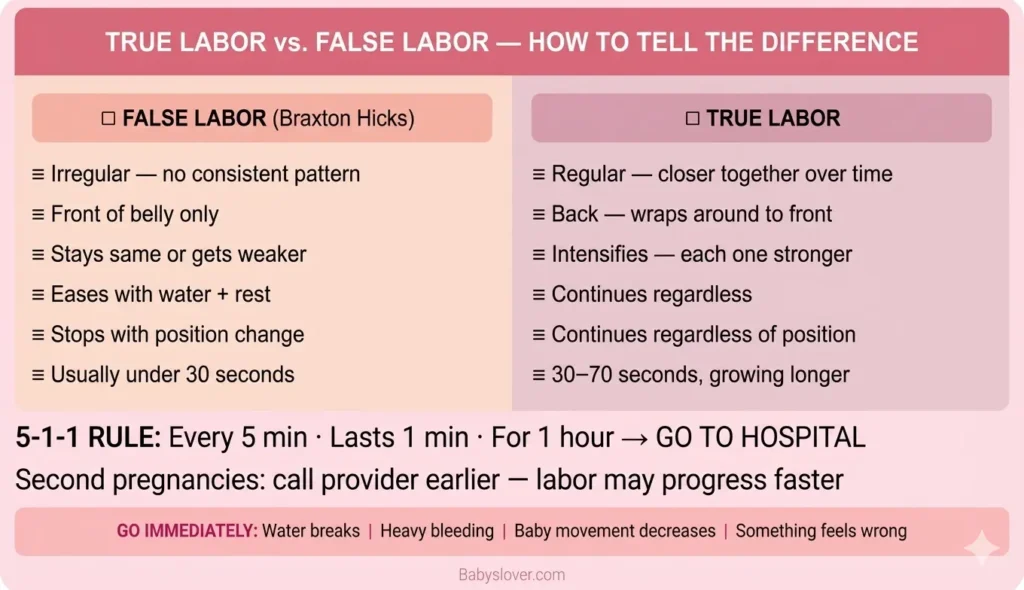
| Feature | False Labor (Braxton Hicks) | True Labor |
| Contraction timing | Irregular – no consistent pattern | Regular – coming closer together over time |
| Contraction location | Front of belly only – no back involvement | Starts in the lower back and wraps around to the front |
| Contraction intensity | Stays the same or decreases | Intensifies steadily over time – each one stronger |
| Duration | Variable – under 30 seconds, sometimes longer | 30-70 seconds each, lengthening over time |
| Response to movement | Often stop when you change position or walk | Continue regardless of position, walking, or rest |
| Response to hydration | Often ease after drinking water and lying down | Not affected by hydration |
| Progression | Does not progress to closer and stronger | Gets closer (5-1-1 rule) and stronger over hours |
| Cervical change | No cervical change on exam | Cervical effacement and dilation progressing |
The 5-1-1 Rule:
Most providers use the 5-1-1 rule as the guideline for when to come to the hospital:
- Contractions every 5 minutes
- Each lasting at least 1 minute
- For at least 1 hour
For first-time mothers, this rule is appropriate. For women in their second or subsequent pregnancy, labor can progress faster – call your provider earlier rather than later.
Always go immediately if:
- Your water breaks – regardless of contractions
- You have heavy bleeding
- Baby’s movements significantly decrease
- You feel something is wrong – trust your instinct
Nutrition at 36 Weeks Pregnant
| Nutrient | Why It Matters at Week 36 | Daily Target and Sources |
| Protein | Baby gaining ~8-12 oz/week – final fat deposits and muscle mass | 71g+ daily – chicken, eggs, Greek yogurt, lentils, cottage cheese |
| Healthy fats | Final fat accumulation at cheeks and shoulders – dietary fat supports this directly | Avocado, olive oil, nuts, fatty fish, full-fat dairy |
| Iron | Blood volume at peak – anemia at this stage causes significant delivery complications | Red meat, lentils, spinach + vitamin C always paired together |
| DHA (Omega-3) | Brain myelination and synaptogenesis continuing through birth | Salmon, sardines, eggs, prenatal vitamins with DHA |
| Fiber + Water | Constipation and hemorrhoids – prevention far easier than treatment now | Prunes, oats, beans, vegetables + 8-10 glasses water daily |
| Calcium | Baby’s bone density still building – adequate intake protects your own bones | Dairy, fortified plant milks, almonds, sardines with bones |
Appetite may improve if your baby has engaged and released some pressure from your stomach. Take advantage of this window to eat nutrient-dense foods while you can. After delivery and with a newborn, nutrition often becomes the first thing neglected – building your stores now matters.
Partner Tips for Week 36
- If an ECV is scheduled, attend. It is a procedure that works best with emotional support present, and the decision-making process that may follow benefits from a partner being informed.
- Know the 5-1-1 rule by heart – and know that for second pregnancies, you may be going to the hospital earlier than this
- Know where the hospital entrance is at 2am – many hospitals have different overnight entrances than daytime ones
- Finalize logistics for any older children or pets – who handles what if labor begins suddenly
- The hospital bag needs to be in the car, not just packed. At 36 weeks, labor could begin any day.
- Know the GBS result – if positive, you need to help ensure early hospital arrival for adequate antibiotic coverage
- Be emotionally present. The final weeks of pregnancy carry anxiety, physical exhaustion, and a strange mix of readiness and fear. Just asking how she is feeling – and actually listening – is more valuable than most practical tasks.
36 Weeks Pregnant Checklist
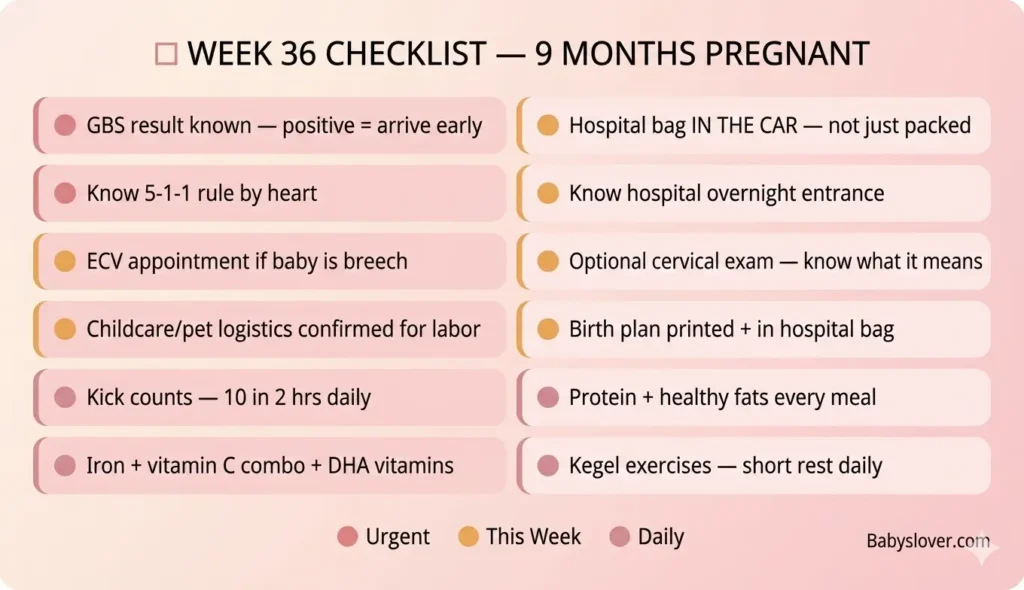
| Task | Priority |
| Know your GBS result and what positive means for labor arrival time | URGENT |
| Hospital bag IN THE CAR – not just packed | URGENT |
| Know the 5-1-1 rule + when to call for second-time moms | URGENT – know this now |
| Know hospital directions + overnight entrance location | URGENT |
| Continue kick counts – 10 movements in 2 hours, daily | Daily |
| ECV appointment if baby is breech – this week or next is the window | If applicable – urgent |
| Optional cervical exam – understand what results do and don’t mean | At this week’s appointment |
| Finalize childcare/pet care arrangements for labor day | This week |
| Birth plan printed and in hospital bag | Confirm this week |
| Know meconium in amniotic fluid – what green-tinged fluid means | Awareness |
| Continue perineal massage 1-2x per week | Weekly |
| Protein + healthy fats at every meal | Daily |
| Iron + vitamin C + DHA prenatal vitamins | Daily |
| Kegel exercises – 3 sets of 10 | Daily |
| Short rest daily – recovery now matters | Daily |
Frequently Asked Questions – 36 Weeks Pregnant
What trimester is 36 weeks pregnant?
36 weeks pregnant is the ninth week of the third trimester. Third trimester runs from Week 28 through Week 40. You have approximately 4 weeks remaining until your due date.
How many months is 36 weeks pregnant?
At 36 weeks pregnant, you are 9 months pregnant. The full 40-week pregnancy spans approximately 9.5 calendar months, which is why most women feel they are ‘more than 9 months pregnant’ by the time their due date arrives.
How much does a baby weigh at 36 weeks pregnant?
At 36 weeks pregnant, your baby weighs approximately 2.6 to 2.9 kg (about 5.7 to 6.4 lbs) and measures around 47-48 cm from head to heel – roughly the size of a large romaine lettuce or papaya. Baby is still gaining approximately 8-12 oz per week.
Is 36 weeks full term?
No – 36 weeks is not full term. According to ACOG classification, 36 weeks is the final week of the preterm window (preterm is before 37 weeks). Early term is Weeks 37-38, and full term – the optimal window – is Weeks 39-40. While a baby born at 36 weeks has an excellent survival rate and will likely do well, meaningful developmental phases including final brain connectivity, fat deposition, and liver maturation continue through Week 39.
What is ECV for a breech baby at 36 weeks?
External Cephalic Version (ECV) is a procedure where a provider manually turns a breech baby to a head-down position by applying pressure to the outside of the abdomen. It is performed at 36-37 weeks in a hospital setting, is successful approximately 50-65% of the time, and carries a low but real risk profile. It is always done with monitoring equipment and the ability to perform emergency delivery if needed.
How do I know if I’m in labor at 36 weeks?
True labor contractions are regular (getting closer together over time), wrap from the lower back around to the front, intensify with each one, and do not stop with position change or hydration. False labor (Braxton Hicks) is irregular, front-focused, and eases with rest and water. The 5-1-1 guideline – contractions every 5 minutes, lasting 1 minute, for 1 hour – is the standard threshold for going to the hospital for first-time mothers. Always go immediately if your water breaks, you have significant bleeding, or baby’s movement decreases.
What is meconium and when does my baby pass it?
Meconium is your baby’s first bowel movement – a dark, greenish-black, tarry substance that forms in the intestines during pregnancy from swallowed amniotic fluid, vernix, lanugo, and bile. It is fully accumulated by around Week 36 and is typically passed within the first 24-48 hours after birth. If meconium is passed before birth (in utero), it can turn the amniotic fluid greenish-brown – called meconium-stained fluid – which requires evaluation at delivery but is common and manageable.
Why does my baby’s head look pointed at birth?
A pointy or asymmetrical head at birth is caused by skull molding – the natural process by which the six flexible bone plates of the skull overlap and compress during passage through the birth canal. This temporarily reduces the skull’s circumference, making delivery possible. The skull returns to its normal rounded shape within hours to days. Babies born by planned cesarean section without labor typically have rounder heads at birth because their skulls were not compressed.
Looking Ahead: 37 Weeks Pregnant
At 37 weeks pregnant, your baby reaches early term status. The final coating of vernix may begin being reabsorbed into the amniotic fluid as it thins. Lungs are at full functional maturity. And the weeks ahead – whether labor comes at 37 or 39 or 41 weeks – will bring the moment this entire journey has been building toward.
Four weeks. A skull ready to mold. Meconium waiting. A complete human being. Keep going.
Follow our pregnancy week by week guide for every development from now to delivery.