

Your due date is today. You have carried a human being through 40 Weeks Pregnant of becoming. Through the weeks of invisibility before anyone could see a bump, through the exhaustion and the nausea and the scans and the appointments and the 3am bathroom trips and the leg cramps and the heartburn and the waiting. All of it has led to this day.
And your baby may not arrive today. That is not a failure of your body or your baby. It is simply how birth works.
Only 5% of babies are born on their due date. The due date you have been counting toward for 40 weeks is a statistical midpoint – the center of a distribution that runs from 38 to 42 weeks. Eighty percent of spontaneous births happen within two weeks either side of this date. Yours may be today, tomorrow, or ten days from now. All of these are within the normal range of human birth timing.
Here is what is happening with your baby, your body, and everything that comes next at 40 weeks pregnant.

Contents
- 1 Quick Summary: 40 Weeks Pregnant
- 2 What’s Happening in Your Body at 40 Weeks Pregnant
- 3 Baby Development at 40 Weeks Pregnant
- 4 The Due Date Is a Midpoint, Not a Deadline
- 5 The Placenta at 40 Weeks – What ‘Post-Dates’ Actually Means
- 6 40 Weeks Pregnant Symptoms
- 7 The Membrane Sweep – What It Is and What to Expect
- 8 The Bishop Score – What Your Provider Is Measuring
- 9 What Happens If You Go Past 40 Weeks – The Monitoring Schedule
- 10 The Three Stages of Labor – Complete Overview
- 11 A Note on the Journey That Ends Here
- 12 Nutrition at 40 Weeks Pregnant
- 13 Partner Tips for Week 40
- 14 40 Weeks Checklist Pregnant
- 15 Frequently Asked Questions – 40 Weeks Pregnant
- 16 This Is the End of Your Pregnancy Week by Week
Quick Summary: 40 Weeks Pregnant
| Detail | Info |
| Baby size | Small pumpkin – ~51-52 cm, ~3.2-3.9 kg (7-8.5 lbs) |
| Trimester | Third trimester – Week 13 of T3 / Due Date Week |
| Term status | Full term |
| Weeks remaining | Due date is today – but most babies come in the next 1-14 days |
| Top milestone | Your due date – the end of a 40-week journey |
| This week’s action | Know post-dates monitoring plan + understand membrane sweep + stages of labor |
What’s Happening in Your Body at 40 Weeks Pregnant
At 40 weeks pregnant, your body is doing one of two things: it is in labor, or it is building toward labor with increasing urgency. The cervix that was thick and closed at Week 36 has been gradually changing for weeks. Effacement and dilation may have been progressing at every appointment. The head that pressed on your pelvis at Week 37 has been pressing further.
Every day at this stage, your provider is watching the same things: your blood pressure, your baby’s movement, the amniotic fluid level, the placenta’s function. The placenta that has sustained your baby for 40 weeks has a lifespan – and after 40 weeks, the monitoring of that lifespan becomes more active.
Your cervix is now the main subject of conversation at weekly appointments. Your provider will track effacement (how thinned), dilation (how open), station (how far down the baby’s head is), and position (how far forward the cervix has moved). These measurements together produce a Bishop score – a number that tells your provider how ready your cervix is for labor or induction.
What to expect at your Week 40 appointment:
- Blood pressure, urine protein – preeclampsia remains a concern until delivery
- Fundal height
- Baby’s heartbeat
- Non-stress test (NST) – heart rate monitoring, 20-40 minutes
- Amniotic fluid index (AFI) – ultrasound measurement of fluid volume
- Cervical exam – Bishop score assessment
- Discussion of membrane sweep – offered at 40 weeks in most guidelines
- Induction planning – date and method, if you have not already discussed
- What happens if you reach 41 weeks – the post-dates monitoring schedule
Baby Development at 40 Weeks Pregnant

At 40 weeks pregnant, your baby measures approximately 51-52 cm from head to heel and weighs around 3.2 to 3.9 kg – often described as the size of a small pumpkin, though individual birth weights vary considerably. Your baby’s exact weight will not be known until they are born and placed on the scale.
| Detail | Measurement |
| Length | ~51-52 cm (about 20 inches) |
| Weight | ~3.2-3.9 kg (approx. 7-8.5 lbs) – varies widely |
| Size comparison | Small pumpkin |
| Term status | Full term |
| All systems | Complete and ready |
At 40 weeks, your baby is ready:
- All organs fully developed: Every major organ system – cardiac, pulmonary, hepatic, renal, neurological, digestive, immunological – is fully developed and operational. The body your baby will live in for the rest of their life is assembled and waiting for its first breath.
- Lungs: final surfactant reserves complete: The alveoli are coated with surfactant. The first breath will inflate them. The second breath will hold them open. The breathing pattern that will sustain life for decades will begin within seconds of birth.
- Brain: primed for birth and the newborn period: The neural connections laid down in the final connectivity sprint are dense and functional. Your baby’s brain is already wiring for recognition – your voice will be familiar from the first moment of hearing it.
- Immune system loaded with maternal antibodies: The placental antibody transfer completed in the final weeks has given your baby the most comprehensive passive immunity it will receive. This protection will last three to six months while your baby’s own immune system begins its independent operation.
- Digestive system queued: Meconium is complete. Enzyme systems are assembled. The sucking, swallowing, and digestion sequence is ready for activation at the first feeding.
- Skin: opaque, thickened, acid mantle forming: The skin your baby will be born with is ready for the world. The acid mantle that will protect against pathogens is beginning to form from birth. Any vernix remaining in the skin creases continues to offer protection.
- The hair question: Some babies are born with a full head of dark hair. Others are born bald. Both are completely genetically determined and entirely normal. Whatever hair your baby has at birth may or may not reflect their eventual hair color or texture.
The Due Date Is a Midpoint, Not a Deadline
The due date calculated from your last menstrual period (or adjusted from ultrasound dating) is based on an average. The average pregnancy duration from the first day of the last period is 280 days – 40 weeks. But this average has a distribution around it.
| Timing | % of Spontaneous Births | What It Means |
| Before Week 37 | ~10% | Preterm birth – requires monitoring and possibly NICU |
| Week 37-38 | ~17% | Early term – healthy but increased risk of some complications |
| Week 39-40 (Full Term) | ~44% | Optimal timing – best outcomes |
| Week 40-41 | ~19% | Full term – still normal, increased monitoring |
| Week 41-42 | ~9% | Late term – monitoring intensifies, induction discussed |
| Beyond Week 42 | ~1% | Post-term – induction strongly recommended |
Looking at this table, you can see that being 40 weeks pregnant and not in labor places you squarely in the normal range. The most common birth timing is 39-41 weeks. Going to 41 weeks is a normal pregnancy trajectory, not a problem to be solved.
What changes as weeks pass is the level of monitoring. Not because something is necessarily wrong – but because the placenta has a finite lifespan, and ensuring it is still functioning optimally becomes more important after 40 weeks.
The Placenta at 40 Weeks – What ‘Post-Dates’ Actually Means
The placenta is one of the most remarkable organs in the human body – and like all organs, it ages. Understanding placental aging is key to understanding why post-dates monitoring matters and why induction is recommended before 42 weeks in almost all guidelines.
The placenta begins as a highly vascular, efficient transfer organ – delivering oxygen, nutrients, and antibodies from your bloodstream to your baby’s. From approximately Week 40 onward, placental function begins to gradually decline. Calcification increases. Blood flow efficiency decreases. The placenta becomes progressively less effective at its primary job.
| Week | Placental Status | Monitoring Frequency |
| 38-40 weeks | Fully functional – optimal | Weekly appointments |
| 40-41 weeks | Beginning gradual aging – still effective | Weekly appointments + NST |
| 41-42 weeks | Aging more noticeably – monitoring critical | Twice-weekly NST + AFI |
| Beyond 42 weeks | Significant aging – induction strongly indicated | Induction recommended by most guidelines |
This is why induction is not offered as a punishment for going overdue – it is offered as a management strategy when the balance between the benefits of additional time in the womb and the risks of placental aging tips in the direction of delivery. The ACOG recommends induction by 42 weeks at the latest, with many providers and guidelines recommending 41 weeks.
40 Weeks Pregnant Symptoms
Everything That Has Been Building Since Week 28
At 40 weeks pregnant, there is not a new symptom list – there is an intensified version of everything that has been accumulating. Pelvic pressure at its maximum. Sleep impossible. Bladder with no capacity. Braxton Hicks strong and frequent. Back pain from the weight of a full-term baby. Heartburn if your baby has not yet engaged. Extreme fatigue.
None of these symptoms are signs that something is wrong. They are the natural consequence of carrying a fully formed human being in a body that was not designed for extended occupancy at this scale. They resolve with delivery – often within hours.
Being Overdue – The Specific Emotional Weight
If your due date has passed and you are still pregnant, there is a specific emotional experience that deserves to be named.
It is not simply impatience. It is the experience of having lived toward a specific date for 40 weeks – of organizing your entire life, your leave, your relationships, your mental preparation around that date – and having the date arrive and pass while you are still waiting. Messages from well-meaning people asking ‘any news?’ accumulate. Your body feels done. Your mind feels done. And the baby is not here yet.
This experience is genuinely difficult. It is not weakness to find it so. The uncertainty of not knowing whether labor is today, tomorrow, or next week – combined with the physical discomfort of full-term pregnancy and the emotional weight of waiting – is a real and significant strain.
What helps: mute your phone. Let a trusted person be the one who takes questions from family and friends and filters out the ‘any news?’ messages. Do things that absorb your attention. Walk every day if your body allows it. Accept that you cannot control the timing – only how you spend the time you have left before the baby arrives.
If you are at 40 weeks and feeling this way, you are not alone, you are not failing, and labor is coming. Every pregnancy ends.
Signs That Labor Is Beginning
At 40 weeks pregnant, every sensation feels significant. Here is how to distinguish what is likely labor from what is likely not.
| Sign | Likely Meaning | What to Do |
| Regular contractions 5 min apart, lasting 1 min, for 1 hour | Active labor – the 5-1-1 rule | Go to hospital |
| Water breaking (gush or trickle that doesn’t stop) | Rupture of membranes – with or without contractions | Go to hospital immediately |
| Bloody show (pink/red mucus) | Cervix is changing – labor likely within hours to days | Note timing, call provider if contractions also present |
| Diarrhea + restlessness + contractions | Early labor beginning | Stay home until 5-1-1, stay hydrated |
| Nesting surge + loss of mucus plug | Body preparing – labor possibly in days | Rest, prepare, stay home |
| Braxton Hicks stopping and starting all day | Prodromal labor – real but not progressive | Rest, hydrate, time them, call if uncertain |
| Baby movement decreasing noticeably | Requires immediate evaluation regardless | Call provider or go to hospital now |
When in doubt at 40 weeks, go in. You will not be judged for coming in and being sent home. It is the appropriate response to uncertainty at full term.
The Membrane Sweep – What It Is and What to Expect
At 40 weeks, most providers will offer a membrane sweep – also called a stretch and sweep. This is one of the most commonly offered procedures at this stage and one of the least explained.
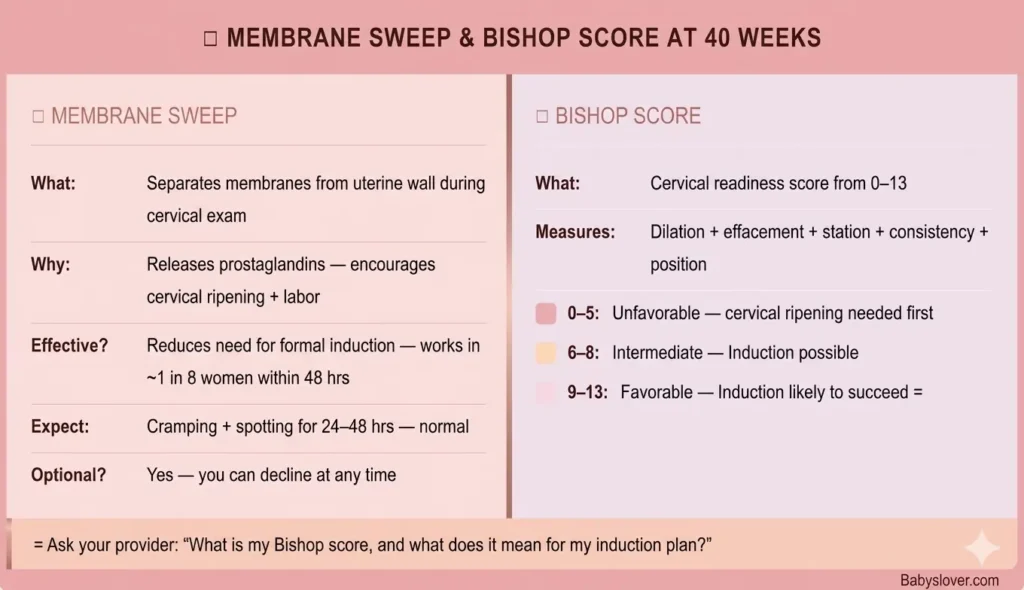
A membrane sweep is performed during a cervical exam. Your provider inserts a gloved finger through the cervix and uses a circular sweeping motion to separate the membranes (the bag of waters) from the lower part of the uterine wall. This contact triggers the release of prostaglandins – the same hormones involved in cervical ripening and labor initiation.
| Question | Answer |
| Does it work? | Research shows membrane sweep increases the likelihood of labor beginning within 48 hours, and reduces the risk of going past 41 weeks. A Cochrane Review found it is effective in reducing the need for formal induction. |
| How effective is it? | Approximately one additional woman in every 8 who receives a sweep will go into labor in the next 48 hours compared to not having one. It doesn’t work for everyone. |
| Does it hurt? | It is uncomfortable – sometimes significantly so – particularly if the cervix is not very dilated. It should not be sharply painful. It takes about 15-30 seconds. |
| What to expect after? | Cramping for a few hours, spotting or bloody discharge for 24-48 hours, and possibly irregular contractions. All of these are normal. |
| When is it offered? | From 40 weeks onward in most guidelines. Some providers offer it at 38-39 weeks. The NICE guidelines recommend offering it at 40 and 41 weeks. |
| Can you decline? | Yes. It is always optional. If you prefer not to have one, you can decline and discuss alternative management plans. |
The Bishop Score – What Your Provider Is Measuring
When your provider performs a cervical exam at 40 weeks pregnant, they are gathering information that adds up to a Bishop score – a number from 0 to 13 (or 0 to 10 in modified versions) that predicts how favorable the cervix is for labor and induction.
The Bishop score is rarely explained to patients despite being used at every late-pregnancy cervical examination. Here is what it measures:
| Factor | 0 Points | 1 Point | 2 Points | 3 Points |
| Dilation (cm) | Closed (0) | 1-2 cm | 3-4 cm | 5+ cm |
| Effacement (%) | 0-30% | 40-50% | 60-70% | 80%+ |
| Station | -3 | -2 | -1 or 0 | +1 or +2 |
| Consistency | Firm | Medium | Soft | – |
| Position | Posterior | Mid | Anterior | – |
| Bishop Score | Cervical Status | Implication |
| 0-5 | Unfavorable cervix | Cervical ripening (prostaglandin gel/insert) typically done before oxytocin induction |
| 6-8 | Intermediate | Induction can proceed with oxytocin; cervical ripening may help |
| 9-13 | Favorable cervix | Induction likely to succeed; oxytocin can start directly |
A high Bishop score at 40 weeks means your cervix is already favorable for either spontaneous labor or induction. A low score means your provider will likely recommend cervical ripening before starting oxytocin – which is why induction at 40 weeks with an unfavorable cervix typically takes longer than induction at 41 weeks with a more ripened cervix.
What Happens If You Go Past 40 Weeks – The Monitoring Schedule
Most pregnancies that have not delivered by 40 weeks will be followed with a specific monitoring plan. Here is the typical schedule:
| Timing | What Typically Happens |
| 40 weeks (today) | Weekly appointment + NST + AFI + cervical exam + membrane sweep offered |
| 40 weeks + 3 days (40+3) | Some providers schedule a second NST or check-in |
| 40 weeks + 7 days (41 weeks) | NST + AFI + biophysical profile (BPP) + second membrane sweep offered + induction planning concrete |
| 41 weeks + 3-4 days (41+3) | Induction strongly recommended or scheduled in most guidelines – ACOG and NICE both recommend not waiting beyond 42 weeks |
| 42 weeks | Post-term – induction or delivery strongly indicated in all guidelines – placental function concerns are significant |
The Non-Stress Test (NST) monitors your baby’s heart rate for 20-40 minutes, looking for accelerations (heart rate increases in response to movement). A reactive NST – which shows two or more accelerations of at least 15 beats per minute lasting at least 15 seconds within 20 minutes – is reassuring. A non-reactive NST prompts further evaluation.
The Amniotic Fluid Index (AFI) uses ultrasound to measure fluid volume in four quadrants of the uterus. Oligohydramnios (too little fluid) can indicate reduced placental function and typically accelerates the induction conversation.
The Three Stages of Labor – Complete Overview
Whether labor begins today or in the next two weeks, understanding what is coming changes how you experience it. Here is the most complete overview in this series.
Stage 1 – Early Labor, Active Labor, and Transition
| Phase | Dilation | Contraction Pattern | Duration | What to Do |
| Early labor | 0 to 6 cm | 5-20 min apart, 30-45 sec each, mild-moderate | Hours (often 6-12+ for first birth) | Stay home. Rest, walk, eat lightly, time contractions. Call provider if uncertain. |
| Active labor | 6 to 10 cm | 3-5 min apart, 45-60+ sec each, strong | Usually 4-8 hours for first birth | Go to hospital. This is when pain relief options are available. Focus on breathing. |
| Transition | 8-10 cm – the final push to full dilation | Every 2-3 min, 60-90 sec each, very intense | Often 15-60 min – the shortest but hardest phase | You are almost there. This phase ends. The pushing urge arrives. |
Stage 2 – Pushing and Birth
From full dilation (10 cm) to delivery. Duration varies enormously – from minutes to hours. You will feel the urge to push when the baby’s head creates pressure on the rectal nerves (the Ferguson reflex). Directed pushing (provider counts, you push on command) and physiologic pushing (pushing when you feel the urge) are both practiced – ask your provider about their approach.
Stage 3 – Delivery of the Placenta
After your baby is born, the placenta must be delivered – typically within 30-60 minutes. Mild contractions continue, your provider may apply gentle cord traction, and you may be asked to push once more. Oxytocin is usually given after delivery to help the uterus contract and reduce bleeding. This stage ends the physical delivery process.
After Stage 3 – The Golden Hour
The first hour after birth – if you and your baby are both well – is for skin-to-skin contact, the breast crawl, the Apgar assessments, and the beginning of bonding. Keep this time as protected and undisturbed as possible. All the routine newborn procedures can wait. These minutes are irreplaceable.
A Note on the Journey That Ends Here
This is the final entry in a series that has followed your pregnancy from Week 1 through Week 40.
It began when your baby was smaller than a period at the end of this sentence. It continued through the weeks of invisible development, through the heartbeat at six weeks, the first kicks at sixteen, the anatomy scan at twenty, the glucose test, the Group B strep swab, the hospital bag, the sleepless nights, the crowded uterus, and the endless waiting.
From Week 1 to Week 40, a complete human being was assembled from a single fertilized cell. Every system. Every reflex. Every feature. The brain that will learn language and remember your face. The lungs that will take their first breath and not stop. The heart that will beat for a lifetime.
You did not do this consciously. Your body knew what to do. You sustained it, nourished it, protected it, and brought it here.
When your baby is placed on your chest – whenever that is, today or two weeks from now – and you feel the weight and warmth of them for the first time, the 40 weeks will compress into a single moment. And then everything that comes after begins.
Every pregnancy ends. Yours will too. And what comes after it is worth every week of the getting here.
Nutrition at 40 Weeks Pregnant
| Nutrient | Why It Still Matters | Best Sources |
| Iron | Postpartum hemorrhage, recovery, and breast milk production all depend on iron stores. Keep building them. | Red meat, lentils, spinach + always pair with vitamin C |
| Protein | Birth recovery – vaginal tearing or cesarean incision require protein to heal. Milk production begins within 24-48 hours. | Chicken, eggs, Greek yogurt, lentils, cottage cheese |
| Healthy fats | Breast milk is 50% fat – your dietary fat composition directly enters the first milk your baby receives | Avocado, olive oil, nuts, fatty fish, full-fat dairy |
| DHA (Omega-3) | Transfers into breast milk. Your baby’s brain development continues and DHA is required for it. | Salmon, sardines, eggs, prenatal vitamins with DHA – continue postpartum |
| Fiber + Water | Post-birth constipation is extremely common, especially after cesarean. Build gut health now. | Prunes, oats, beans, vegetables + minimum 8-10 glasses water daily |
Continue your prenatal vitamins after birth – particularly if breastfeeding. The nutritional demands of producing breast milk are significant, and your body will take what it needs from your own stores if your diet does not provide it.
Partner Tips for Week 40
- If the due date has passed and labor has not started – be patient in a way that she can feel. Not anxious patience. Calm, present, steady patience.
- Know the monitoring schedule – NST, AFI, membrane sweep, Bishop score. Be part of these conversations at appointments.
- Handle the incoming messages from family and friends asking ‘any news?’ – take this entirely off her plate.
- Walk with her. Walking releases oxytocin, helps the baby descend, and moves time.
- If labor begins at 3am, be awake, present, and calm. This is the moment everything has been building toward. Your job is to be there.
- Know the hospital logistics perfectly – parking, entrance, where to go, what to say.
- After the birth: say nothing for the first few minutes. Just witness what has just happened. There will be time for everything else.
- You are about to become a father. Whatever that means to you – whatever version of that you have imagined – it begins the moment that baby arrives. Be ready. Be present. This is what all of it was for.
40 Weeks Checklist Pregnant
| Task | Priority |
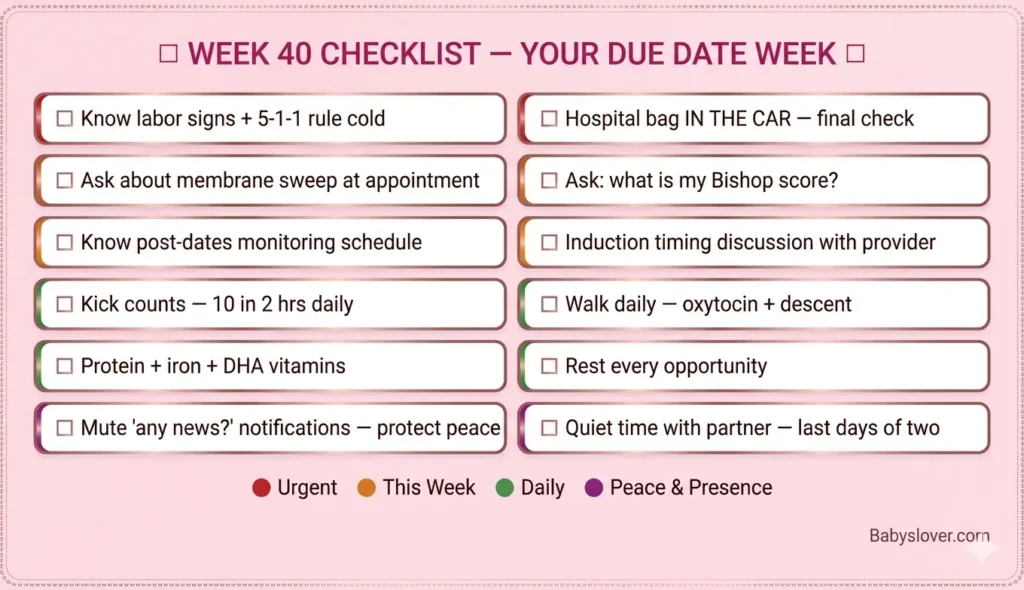
| Know labor signs + 5-1-1 rule – know them cold | URGENT |
| Hospital bag in the car – confirmed one final time | URGENT |
| Know hospital directions + overnight entrance | URGENT |
| Ask about membrane sweep at this week’s appointment | This week |
| Ask your provider about your Bishop score and what it means | This week |
| Know the post-dates monitoring schedule if labor doesn’t start | This week |
| Discuss induction timing and plan concretely with your provider | This week |
| Continue kick counts – 10 movements in 2 hours, every day | Daily |
| Mute notifications from ‘any news?’ sources – protect your peace | Now |
| Walk daily if your body allows – supports descent and oxytocin | Daily |
| Rest every time you can – labor reserves are built in the final days | Daily |
| Protein + iron + healthy fats at every meal | Daily |
| DHA prenatal vitamins – continue through postpartum if breastfeeding | Daily |
| Quiet time with your partner – the last days of two becoming three | This week |
| Birth plan confirmed + in hospital bag + partner has read it | Confirm |
| Newborn safe sleep setup confirmed at home | Confirm |
Follow our pregnancy week by week guide for every development from now to delivery.
Frequently Asked Questions – 40 Weeks Pregnant
Is 40 weeks full term?
Yes – 40 weeks is within the full term window (39-40 weeks 6 days) as defined by ACOG. Full term is the optimal developmental window and the point at which all major organ systems are complete. A baby born at 40 weeks has the best possible developmental foundation. If labor has not started by 40 weeks, this is normal – most births happen between 39 and 41 weeks.
What happens if I go overdue at 40 weeks?
Going past 40 weeks without delivering is common – only 5% of babies are born on their due date. If you reach 40 weeks without labor, your provider will increase monitoring: weekly (or twice-weekly) non-stress tests (NST), amniotic fluid checks (AFI), and biophysical profiles (BPP). A membrane sweep may be offered to encourage labor. Most guidelines recommend discussing induction at 41 weeks, and strongly recommend induction by 42 weeks due to increasing placental aging and stillbirth risk beyond that point.
How much does a baby weigh at 40 weeks pregnant?
At 40 weeks pregnant, babies weigh anywhere from 3.2 to 3.9 kg (about 7 to 8.5 lbs) on average, though healthy birth weights range from around 2.5 to 4.5 kg (5.5 to 10 lbs) in normal term pregnancies. Individual genetics, nutrition, and pregnancy factors all influence birth weight. The actual weight will be known at delivery.
What is a membrane sweep at 40 weeks?
A membrane sweep is a procedure performed during a cervical exam in which your provider uses a gloved finger to separate the membranes (bag of waters) from the lower uterine wall. This triggers prostaglandin release, which can encourage cervical ripening and labor onset. Research shows it reduces the risk of going past 41 weeks and the need for formal induction. It causes cramping and possible spotting for 24-48 hours. It is optional – you can decline.
What is the Bishop score in pregnancy?
The Bishop score is a cervical assessment scored from 0 to 13 based on five factors: dilation, effacement, station, cervical consistency, and cervical position. A score of 0-5 indicates an unfavorable cervix that would benefit from ripening before induction. A score of 6-8 is intermediate. A score of 9 or above is favorable and indicates induction is likely to succeed. Your provider calculates this at every cervical exam and uses it to plan induction approach and timing.
When should I call my provider at 40 weeks?
Call your provider immediately or go to the hospital if: contractions are regular every 5 minutes, lasting 1 minute, for 1 hour (5-1-1 rule); your water breaks; you notice bright red bleeding; your baby’s movements decrease significantly; or you feel something is wrong. At 40 weeks, if you are uncertain whether you are in labor, call and describe what you are feeling. Your provider would rather assess you and send you home than have you wait alone uncertain.
What are the stages of labor?
Labor has three stages. Stage 1 has three phases: early labor (0-6 cm dilation, mild contractions every 5-20 minutes – stay home), active labor (6-10 cm, contractions every 3-5 minutes – go to hospital), and transition (8-10 cm, very intense contractions every 2-3 minutes – the shortest but hardest phase). Stage 2 is pushing and birth, from full dilation until delivery. Stage 3 is delivery of the placenta, typically within 30-60 minutes of birth. The first hour after birth is the golden hour – protect this time for skin-to-skin contact.
This Is the End of Your Pregnancy Week by Week
You have now read through every week of the pregnancy journey – from Week 1, when your baby was an idea and a possibility, through Week 40, when that idea has become a fully formed human being waiting to be born.
This series was built to give you more than generic information – to give you the specific science, the real mechanisms, the honest facts, and the emotional acknowledgment that goes with each stage of this journey. We hope it has done that.
What comes next is beyond what any week-by-week guide can cover. But you are ready. You have done 40 weeks of the most extraordinary thing a human body can do. Whatever happens in that delivery room – however labor unfolds, however long it takes – you have already proven what you are capable of.
From all of us at Babyslover: go meet your baby. For everything from here through delivery, our pregnancy tips for first time moms is with you every step. 💗